Abstract
Immediate placement of dental implant into the fresh extraction socket has been an acceptable procedure for the past two decades. Commonly, immediate placement has been reserved for the single rooted anterior tooth and single or bi-rooted premolar tooth. To preserve the alveolar bone proper, particularly that of the labial and lingual plates of bone it is essential that the extraction should be done in an atraumatic manner, providing the optimal environment for maximizing bone implant contact and implant stability. There is plethora of techniques in the literature for atraumatic extraction of tooth. This paper presents the atraumatic extraction of maxillary premolar by using Sapian root removal device system followed by immediate placement of dental implant.
Key words
atraumatic tooth extraction, immediate implant placement, sapian extraction kit
Introduction
Immediate placement of dental implants into fresh extraction sockets limits overall treatment time and offers some esthetic and functional advantages. It is considered to be advantageous because of several reasons: it shortens the treatment duration, reduces the number of surgical visits, preserves soft tissue and hard tissue architecture, and enhances aesthetic outcome [1-4]. Success of immediate implant placement depends on the crestal bone that is remain after extraction of tooth or tooth root. Atraumatic extraction without jeopardizing the crestal bone level by using numerous devices has been advocated in literature like Periotomes, Powertome periotome 100S (Westport Medical) [5], Golden Misch’s one minute extraction-Physics forceps [6], Meisinger’s Benex control-root extraction system [7] and Easy X-Trac system [8] (Titan Instrument, Hamburg, New York, USA) etc. Amongst these, one of the device is Sapian root removal device system invented by Dr. Schubert Sapian. This case report presents the atraumatic extraction of tooth root by using Sapian root remover system followed by immediate placement of implant in the maxillary left second premolar region and also throws light briefly about the system.
Case report
A 48 year old male patient reported to the department with the chief complaint of missing upper and lower back region teeth and needed replacement. Patient presented history of extraction 3 years back because of decay.
On oral and roengenographic examination (Figures 1-5), it was found that there were missing teeth number 4,15,18,31,32, endodontically treated teeth number 7,8,9 and 10, grossly decayed tooth number 13 and amalgam restoration with teeth number 2 and 14.
Figure 1.Preoperative Frontal view.
Figure 2.Preoperative Maxillary view.

Figure 3.Preoperative Mandibular view.
Figure 4.Orthopentomogram of the patient.
Figure 5.Preoperative Intraoral Periapical X-ray view.
Patient’s occlusion was analyzed and found habitual position of the mandible since centric relation occlusion not coinciding with maximum intercuspation position. There was generalized attrition secondary to physiologic tooth wear resulting in decrease in vertical dimension of occlusion.
Based on the clinical findings and occlusal analysis, treatment plan executed full mouth rehabilitation using Hobo and Takayama’s Twin stage philosophy which reestablish vertical dimension of occlusion and centric relation coinciding with centric occlusion by using porcelain fused to metal crowns followed by immediate implant placement in the region of 13 after extraction of the same using Sapian root removal kit and restored with porcelain fused to metal crown.
After completion of Twin stage approach for the full mouth rehabilitation, patient was appointed for the immediate implant placement in the region of tooth number 13.
Sapian extraction kit was used for the extraction of 13 (Figure 6) and subsequently 3.5 mm*11 mm Ankylos ( Dentsply Int) Implant (Figure 7) and transmucosal extension was installed (Figure 8) and radiograph was taken (Figure 9).
Figure 6. Extracted root piece.

Figure 7.Immediate Implant placement.

Figure 8.Placement of transmucosal extension.
Figure 9.Postoperative Intraoral Periapical X-ray view.
Description of Sapian Root Remover Kit [9] (Figure 10 and 11): The Sapian root remover kit consists of following parts.

Figure 10.Sapian Extraction Kit.
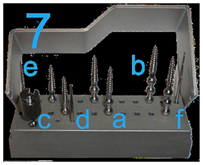
Figure 11.Sapian Extraction Kit: Screws.
- Anterior driver
- Collet nut for anterior driver
- Manual latch head driver
- Pry bar
- Gear oil vial and spout for manual latch head driver
- Extraction screw block with built-in screw straightener
- Solid aluminum screw block containing:
- Three thin extraction screws: one 1-ball, one 2-ball and one 3-ball
- Three thick extraction screws: one 1-ball, one 2-ball and one 3-ball
- Finger driver
- #557 Surgical high speed cutting bur
- 33mm total length RA latch pilot drill
- Fulcrum tray with removable silicone elastomer cushion pad
- Soft silicone pin mat cushion for screw block and fulcrum tray
- Autoclavable stainless steel instrument cassette
Discussion
The Sapian Root Remover System allows dental surgeon to perform an atraumatic root extraction. This type of extraction reduces the healing time and pain associated with other procedures and the same time operated site is also optimized for immediate implant placement. In this paper, author has used Sapian extraction system because of the feasibility of the system and easy manipulation.
First, a pilot hole was prepared in the root to facilitate proper engagement of the Extraction Screw in the root. Choice of a one, two, or three ball Extraction Screw depends on the depth of the root and the clearance within the mouth. When the screw is in the tooth and ready for extraction, the lifting ball on the screw shaft should be 3-4 mm above the occlusal level of the adjacent teeth. The proper choice for the Extraction Screw was determined by comparing it against the radiograph. They are supplied with either thick or thin thread tapers. To permit easy recognition of thin and thick screws, thick screws are marked by a dark band. A thin screw is preferred for situations where the extraction angle or other circumstances necessitate the use a more flexible screw. A thick screw is useful where greater rigidity provides a structural advantage in the extraction mechanics. Some roots will be so severely decayed that the threads of a thin Extraction Screw will not engage firmly in the root. In this case, author has used the thick Extraction Screw that usually has sufficient grasp to remove the root. Depending upon preference and convenience, select either the Anterior Driver or the Manual Latch Head Driver for Extraction Screw placement. Use the Anterior Driver for convenient screw placement in anterior and premolar maxillary teeth. This driver can be used with one hand to place the Extraction Screw with precision, speed and maximum tactile sensitivity. Alternatively, use the Manual Latch Head Driver to place an Extraction Screw in any part of the mouth, including areas that cannot be reached with the Anterior Driver. Proper positioning of the Fulcrum Tray is critical to the success of the extraction. It supports the downward force of the Pry Bar and protects delicate structures. The downward force on the handle of the Pry Bar creates the vertical force that lifts the Extraction Screw. The Fulcrum tray must be positioned to provide maximum support for such downward pressure. Extraction force must be applied in a vertical direction aligned with the root. Align the Pry Bar in a mesial-distal direction to prevent damage to the buccal plate and maximize extraction force. The fulcrum of the Pry Bar on the Fulcrum Tray should be directly over the strongest adjacent tooth, which is usually mesial of the root to be extracted. The extracted root can be removed from the Extraction Screw by using the Finger Driver, the Anterior Driver or the Manual Driver. The Finger Driver is usually the quickest and easiest for this task. Simply hold the root firmly with one hand, preferably with a 2" square gauze pad, and unwind the Extraction Screw with the other hand until the root is released [9].
Conclusion
Immediate surgical and restorative protocols facilitate superior esthetic and functional success. However, strict guidelines for atraumatic intervention and preservation of existing anatomic structures must be carefully followed. This article presented a comprehensive treatment approach and discussed current immediate procedures based on the existing scientific evidence.
References
- Fugazzotto PA (2005) Success and failure rates of osseointegrated implants in function in regenerated bone for 72 to 13 months. Int J Oral Max Impl 20: 77–83.
- Fugazzotto PA (2008) Implant placement at the time of mandibular molar extraction: description of technique and preliminary results of 341 cases. J Periodontol 79: 737–747. [Crossref]
- Fugazzotto PA, Shanaman R, Manos T, Shectman R (1997) Guided bone regeneration in implant therapy: success and failure rates in 1503 sites. Int J Perio Rest Dent 7: 73–76.
- Fugazzotto PA (2004) Guided bone regeneration at immediate implant insertion and loading: a case report. Implant Dent 13:223–227. [Crossref]
- Kang J, Dym H, Stern A (2009) Use of the Powertome Periotome to Preserve Alveolar Bone During Tooth Extraction – A Preliminary Study. Oral Surg Oral Med Oral Pathol and Oral Radiol 108: 524-525.
- Golden RM (2005) inventor; GoldenMisch Inc, assignee. Dental plier design with offsetting jaw and pad elements for assisting in removing upper and lower teeth utilizing the dental plier design. US patent 6,910,890.
- Saund D, Dletrich T (2013) Minimally-Invasive tooth extraction: Doorknobs and strings revisited!. Dent Update 40: 325-330. [Crossref]
- White J, Holtzclaw D, Toscano N (2009) Powertome assisted atraumatic tooth extraction. J Imp and Adv Clin Dent 1: 34-44.
- http://www.SapianRD.com/files/sapianrootremoverinstructions.pdf