Dental identification is one of the primary methods of identifying unknown human remains. It is based upon the comparison of post mortem findings with ante mortem dental records. Comparison of dental radiographs is recognized as integral to this process. In many parts of the world caries rates have fallen and many young people have no restorations. This makes dental identification more challenging and necessitates the comparison of anatomical structures. The aim of this study was to compare the ability of a variety of dentists and forensic toxicologists to correctly match restoration and caries free bitewing radiographs of children taken a number of years apart.
7 sets of radiographs which were taken 4 years apart were given to 22 examiners and were asked to sort them into seven matching pairs. The number of correctly matched pairs, the features used for comparison and the time taken for the matching was recorded. A comparison between the different groups was made. Of the potential 154 matched pairs of radiographs, a total of 115 pairs were identified correctly. The senior clinicians, recently qualified dentists, post graduate dental students and forensic specialists correctly identified 71.5%, 77%, 78.5% and 71.5% matches respectively. This simulated radiographic identification test may identify that clinical experience is not related to making correct matches. Formal training in dental identification might be helpful, so that dentists of varied experience levels (seniors &juniors) and forensic specialists can take part in an identification team when needed.
dental identification, bitewing radiographs, caries free teeth, anatomical features, radiographic and clinical experience
Various methods, including teeth, fingerprints and DNA that compare ante mortem data with post mortem findings are employed in the identification of unknown human remains. Teeth are the hardest structures of the human body, highly resistant to heat and putrefactive changes. No matter how poor the condition of the body, it is likely that the teeth will be better preserved than the other structures that are used as primary sources of identification [1]. Therefore, teeth are important and often the most reliable comparative tool in identification [2-4]. The collection of ante mortem dental records does not rely on specialist equipment or staff and may, therefore, be easier to obtain than other ante mortem data, such as fingerprints [5]. Compared to other means of identification, dental identification was relatively simple, quick and low cost [6]. For these reasons dental comparisons is widely regarded as a method of choice in identification [7]. Forensic dental identification is also accepted as one of the primary means of identification by the International criminal police organization (INTERPOL) along with fingerprint and DNA analysis [8].
A variety of sources of ante mortem dental evidence are available, including treatment notes, dental charts, radiographs, cast and photographs. Dental radiographs, which provide a clear detail of odontoskeletal findings of the individual [9] are one of the most accurate and powerful sources of dental ante mortem information. During the past two decades, there has been a significant decrease in caries rate in many countries because of improved dental care and water fluoridation [10,11]. If there is no evidence of dental intervention, then the forensic dentist must rely on anatomical structures common between ante mortem and post mortem radiographs. These features include crown morphology, pulpal morphology, root shape and curvatures, spacing between teeth and bony trabecular pattern [12].
There has been various studies that are carried out in the past in order to test the observer’s accuracy and to what extent their education, experience and training aids in the outcome of the post mortem & ante mortem radiographic comparison. Sholl, Moody [7] concluded that there is poor correlation between knowledge of the examiner and outcome, formal training is highly desirable. Kogon, MacLean [13] suggested that there is significant reduction in accuracy of identification by the observers with increased time intervals between the radiographs. Pinchi et al., [14] reported that cognitive bias is the possible source of outcome variability between dentists who received formal training in forensic odontology and those who didn’t.
Even with improving technology and development of computer aided methods, most of the studies on forensic dental identification by comparison are relied on operator’s decision making. Various dental radiographs have been utilized such as intra oral periapical radiographs (IOPA), bite wing radiographs and Orthopantamograms (OPG). Even non dental radiographs were also proved helpful in identification [15]. Kogon and MacLean [16] supported the continued use of bite wing radiographs for identification. Bite wing radiographs are used by dentists to detect proximal caries, and are considered to be the most commonly taken radiograph [17]. This study investigates the reliability of radiographs for dental identification when no restorations are present.
This study aims to compare the ability of a variety of dentists and other forensic personnel to correctly match the bitewing radiographs of children. Caries free radiographs were included to increase the complexity of the study.
The study was designed to positively match the provided bitewing radiographs. The examiners were provided with 7 sets of radiographs, which include 7 simulated ante mortem bitewing radiographs (AM- BWs) and 7 simulated post-mortem ones (PM- BWs). For each set bitewing radiographs were taken from both right and left sides (In total 28 BWs, i.e., 14 AM- BWs & 14 PM- BWs). The radiographs were taken as part of routine care during a clinical trial of children in the 1990’s. The details of the children was not provided to the examiners and kept confidential. The time interval between the simulated ante and post mortem radiographs varied from 3 to 4 years. All films were taken using a standardized parallel film technique with a film holder (Kwik bite, Hawe Neos Dental, Bioggio, Switzerland) and ultra speed film (Eastman Kodak Company, Rochester, N.Y., USA). Although the films were not always exposed using the same x-ray unit, quality assurance procedures ensured consistent quality radiographs.
The AM- BWs were labelled with letters from A to G, while the PM- BWs were labelled with numbers 1 to 7. Examiners were asked to provide which PM-BW number matched to which AM- BW letter. The examiners were given only chance to do the match and were requested to do all the matches. The examiners were not given any time limit and were not informed that the time taken for identification was being recorded. Presence of any restorations in the radiographs would have made the identification easier. To further intricate the study, caries free bitewing radiographs were chosen. These radiographs exhibit not only just teeth but also other anatomical features which will be helpful for comparison.
Twenty two volunteer examiners were asked to pair the radiographs. They were divided into groups and named as follows
- SDC (n=6) Senior dental clinicians, they all are working in same dental hospital with no training in forensic odontology
- JDC (n=5) Junior dental clinicians with experience ranging from 1 to 3 years and with no training in forensic odontology
- PG (n=6) Post graduate dental students who are acquiring training in clinical dentistry including two forensic odontology students
- FSP (n=5) Forensic specialists having experience in legal medicine (mainly forensic pathology & forensic toxicology)
Examiners were asked how easy they found the task overall on a scale of 1-10. An examination protocol and a dedicated scoring sheet were developed, trialled and amended prior to the study proper using 4 subjects. The clinical experience of the volunteers ranged from 4 to 20 years. Time taken for the completion of matching was noted down separately. After the examiner had confirmed each pairing they were asked to determine which radiographic (anatomic) features were most helpful in making the identification. Reasons for identification were recorded separately on the scoring sheet.
The responses of each group of examiners were evaluated on the basis of
- The number of correct matches for each set of radiographs
- Time taken for the identification process
- Difficulty scale
- Accuracy of volunteer examiners
Of the total 154 matched pairs of radiographs a total of 115 pairs was identified correctly. The total number of correct matches was 75%. The number of correct matches done by each examiner and the time taken were recorded Table 1. Table 2 lists the percentage of correct responses for each group of examiners for each set of radiographs. The SDC, JDC, PG and FSP correctly identified with 71.5%, 77%, 78.5% and 71.5% respectively.
Table 1. Number of correct matches and time taken by each examiner
Examiner |
Correct matches |
Time taken |
senior 1 |
7 |
18 min |
Senior 2 |
5 |
12 min |
Senior 3 |
4 |
19 min |
Senior 4 |
2 |
14 min |
Senior 5 |
5 |
16 min |
Senior 6 |
7 |
22 min |
Qualified dentist 1 |
3 |
15 min |
Qualified dentist 2 |
7 |
16 min |
Qualified dentist 3 |
7 |
16 min |
Qualified dentist 4 |
5 |
18 min |
Qualified dentist 5 |
5 |
20 min |
Post graduate 1 |
7 |
19 min |
Post graduate 2 |
5 |
18 min |
Post graduate 3 |
2 |
28 min |
Post graduate 4 |
7 |
18 min |
Post graduate 5 |
7 |
19 min |
Post graduate 6 |
5 |
20 min |
Forensic toxicologist 1 |
2 |
10 min |
Forensic toxicologist 2 |
7 |
28 min |
Forensic toxicologist 3 |
4 |
15 min |
Forensic toxicologist 4 |
5 |
19 min |
Forensic toxicologist 5 |
7 |
21 min |
Table 2. Accuracy of Identification
|
Group 1 |
Group 2 |
Group 3 |
Group 4 |
Total Correct |
Set A |
5/6 83% |
4/5 80% |
5/6 83% |
2/5 40% |
16/22 72% |
Set B |
3/6 50% |
4/5 80% |
3/6 50% |
4/5 80% |
14/22 64% |
Set C |
2/6 33% |
3/5 60% |
4/6 67% |
4/5 80% |
13/22 59% |
Set D |
3/6 50% |
3/5 60% |
4/6 67% |
2/5 40% |
12/22 54.5% |
Set E |
6/6 100% |
5/5 100% |
6/6 100% |
5/5 100% |
22/22 100% |
Set F |
5/6 83% |
4/5 80% |
6/6 100% |
4/5 80% |
19/22 86.3% |
Set G |
6/6 100% |
4/5 80% |
5/6 83% |
4/5 80% |
19/22 86.3% |
Total Correct |
30/42 71.5% |
27/35 77% |
33/42 78.5% |
71.5% 25/35 |
115/154 75% |
The difference in the accuracy of responses of group 1 and group 2 (P=0.86), group 1 and group 3 (P=0.87), group 1 and group 4 (P=0.77), group 2 and group 3 (P=0.75), group 2 and group 4 (P=0.90) and group 3 and group 4 (P=0.66) were not statistically significant.
- Time taken for identification
The time taken by each examiner for identification was recorded without the knowledge of the examiner in order to avoid bias. The average time taken by volunteer examiners was 18.2 minutes with a maximum of 28 minutes and a minimum of 10 minutes. The time taken for identification by each examiner is given in Table 1.
The average time taken was 16.8 minutes for SDC, 17.0 minutes for JDC, 20.3 minutes for PG dental students and 18.6 minutes for FSP. There is no statistical significance in the time taken between the groups. Table 3 lists the average time taken and accuracy of identification by each group.
Table 3. Comparison between average time consumption and accuracy of identification
|
Average time taken |
Accuracy of identification |
Group 1 (senior clinicians) |
16.8 minutes |
71.5% |
Group 2 (Qualified dentists) |
17 minutes |
77% |
Group 3 (PG dental students) |
20.3 minutes |
78.5% |
Group 4 (For.tox’gists) |
18.6 minutes |
71.5% |
- Difficulty scale
Examiners were asked to rate how difficult or easy this identification process was. On a scale of 1 to 10, 1 stands for very easy and 10 stand for very difficult. Five examiners gave a difficulty rating average of 5 or less. The remaining 17 examiners felt that it was a difficult task and rated more than five. Only one examiner rated 10/10 and found it very difficult. The examiner who rated the task as most difficult also made the maximum number of mismatches (only 2 correct).
- Comparing individual sets of radiographs
Among the 7 sets of radiographs, Set E radiograph was correctly matched by all the 22 examiners (100%). Normally mixed up pairs throughout the identification study was set C & set D, with correctly matching percentages 59% and 54.5%. Details were provided in Table 2.
- Reasons for matching
Examiners participated in the study believed that crown morphology, pulp morphology and root outline are the greatest aids in matching. Table 4 lists the radiographic features which were used by examiners for matching.
Table 4. Reasons for matching (Identification features)
Group 1 |
Group 2 |
Group 3 |
Group 4 |
-Crown morphology
-Root outline
-Pulp horns
-Combination of small rotations of teeth
-Spacing between teeth |
-Crown morphology
-Pulp morphology
-Root outline
-Angulation of teeth
-Spacing between teeth |
-Crown morphology
-Pulp morphology
- Combination of small rotations of teeth
-Root outline
-Eruption pattern
-Missing teeth |
-Pulp morphology
-Root outline
-Angulation of teeth
-spacing between teeth |
- Radiographs used in this study
Dental radiography is the integral part of reconciliation process of mass fatality incidents. It provides objective evidence of the dentition before and after death [18]. They are classified by the method of acquisition which is either digital or conventional. Among them digital radiography got an edge over conventional because of its low radiation exposure, no chemical processing and it facilitates easy storage [19]. It was successfully used by the forensic odontologists in disaster victim identification following tsunami in 2004 [20]. This experiment doesn’t utilized digital images, but may be incorporated into future investigations.
Possibly, this experiment doesn’t simulate the real dental identification but the radiographs which were taken years apart indeed simulated the true practice of forensic dental identification.
- Examiners, their clinical experience and outcome
The examiners included are qualified dentists and forensic personnel, in which the former were sub categorized into three groups based on clinical experience and latter into forensic pathologists and forensic toxicologists. None of the examiners got any experience in dental identification. During disasters of large scale because of more number of fatalities, participation of non-specialists happens in identification process [21]. As it was already proved in earlier studies that forensic dentists outperformed other examiners [13,16] in identification this experiment carried with general dentists and other forensic personnel thus excluding experienced forensic dentists. But two examiners who are sooner to be forensic dentists were included in order to determine whether training matters in dental identification or not.
The results among the groups of dentists are quite interesting. The Post graduate dental students outperformed Senior (SDC) and Junior (JDC) dental clinicians. This performance of PG students can be explained by Hawthorne effect. This is a type of reactivity in which individuals modify or improve an aspect of their behavior in response to their awareness of being observed [22]. When the examiners are aware of being observed or evaluated, they tend to perform better than other examiners. This commitment of the students did explain the outcome of this experiment.
On the other hand, dental clinicians (both SDC& JDC) with clinical experience performed slightly lower to PG dental students. There is no statistical significance present between groups in relation to the time taken, but more accurate identification is related to increasing time taken. It had shown that those groups which had taken more time for comparison did perform better than those who do not (Figure 1). This might explain the outcome of SDC & JDC. Compared to PG’s they had taken less time for comparison. This experiment suggests that a minimal training is necessary for the dentists irrespective of their clinical experience. Radiographic experience of the dentists is more vital than the clinical experience. Several studies also agreed that the accuracy of dental identification increases with radiographic experience [23].
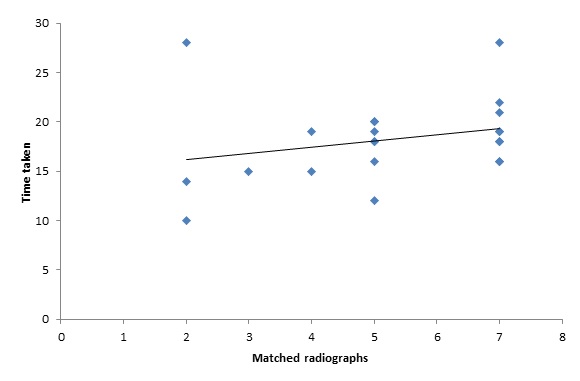
Figure 1. Plot of correct matches agains2021 Copyright OAT. All rights reserv
- Method of approach for matching
The examiners used a wide variety of approaches to pairing the radiographs: crown morphology, pulp morphology and root alignment. The results are similar to those of Sholl [7] who reported that root morphology and alignment had been the greatest aids in matching. In addition, this study has demonstrated that examiners who did pairing based on multiple anatomical features rather than one identified more correct pairings.
The accuracy of identification also varied among the 7 sets of radiographs. Set E radiographs were correctly matched by all the examiners (100% accuracy rate). This is because of the spacing between the teeth and missing tooth. Set D was most commonly mismatched and this has been most often with set C. Their matching percentages were 59% and 54.5% (Table 2). These pairs of radiographs were nearly identical, with only minor anatomical differences. The examiners who correctly identified these 2 sets of radiographs made their conclusions on the basis of 2 or more anatomical features instead of one highlighting the importance of such a strategy.
- Possible improvements
In this study, similar number of post mortem and ante mortem radiographs was utilized and identification was carried by the comparison of single ante mortem and post mortem records. Because of this if one pair is incorrectly matched a second one is also incorrect. Only matching ante mortem and post mortem radiographs were given and no non- matching radiographs were included. It was therefore only possible to get either 100% or 71% (or less if fewer than 5 sets were matched). Many of the examiners did 5 correct matches out of the 7 sets of radiographs. Less number of radiographs was utilized and more needed to deal with in future investigations.
This study differed from real forensic dental identification in that it was limited to bitewing radiographs. Forensic dentists can and will use all other forms of dental records such as treatment notes, odontograms, casts, photographs and other data that are available to them to provide an identification [9]. Therefore, the results should not be taken as indication for accuracy of dental identification as a whole.
This study has proven that radiographic experience is more important than clinical experience of the dentists. Crown morphology, pulp morphology and root alignment were the most commonly used features for matching. The results also support the need for trained radiographic interpreters in forensic dental identification.
- Whittaker DK, Rawle LW (1987) The effect of conditions of putrefaction on species determination in human and animal teeth. Forensic Sci Int 35: 209-212. [Crossref]
- McKenna CJ (1999) Radiography in forensic dental identification--a review. J Forensic Odontostomatol 17: 47-53. [Crossref]
- Pretty IA, Sweet D (2001) A look at forensic dentistry--Part 1: The role of teeth in the determination of human identity. Br Dent J 190: 359-366. [Crossref]
- Pretty IA (2007) Forensic dentistry: 1. Identification of human remains. Dent Update 34: 621-622, 624-6, 629-30 passim. [Crossref]
- Avon SL (2004) Forensic odontology: the roles and responsibilities of the dentist. J Can Dent Assoc 70: 453-458. [Crossref]
- Pinchi V, Zei G (2008) Two positive identifications assessed with occasional dental findings on non-dental x-rays. J Forensic Odontostomatol 27 (2): 34-38. [Crossref]
- Sholl SA, Moody GH (2001) Evaluation of dental radiographic identification: an experimental study. Forensic Sci Int 115: 165-169. [Crossref]
- Hill AJ, Hewson I, Lain R (2011) The role of the forensic odontologist in disaster victim identification: lessons for management. Forensic Sci Int 205: 44-47. [Crossref]
- Adams BJ (2003) Establishing personal identification based on specific patterns of missing, filled, and unrestored teeth. J Forensic Sci 48: 487-496. [Crossref]
- Singh KA, Spencer AJ (2004) Relative effects of pre and post eruption water fluoride on caries experience by surface type of permanent first molars. Commun Dent Oral Epidemiol 32: 435-446. [Crossref]
- Marthaler TM (2004) Changes in dental caries 1953-2003. Caries Res 38: 173-181. [Crossref]
- Wood RE (2006) Forensic aspects of maxillofacial radiology. Forensic Sci Int 159 Suppl 1: S47-55. [Crossref]
- Kogon SL, MacLean DF (1996) Long-term validation study of bitewing dental radiographs for forensic identification. J Forensic Sci 41: 230-232. [Crossref]
- Pinchi V, Norelli GA, Caputi F, Fassina G, Pradella F, et al. (2012) Dental identification by comparison of antemortem and postmortem dental radiographs: Influence of operator qualifications and cognitive bias. Forensic Sci Int 222: 252-255 [Crossref]
- Birngruber CG, Obert M, Ramsthaler F, Kreutz K, Verhoff MA (2011) Comparative dental radiographic identification using flat panel CT. Forensic Sci Int 209: e31-34. [Crossref]
- MacLean DF, Kogon SL, Stitt LW (1994) Validation of dental radiographs for human identification. J Forensic Sci 39: 1195-1200. [Crossref]
- Kogon SL, McKay AE, Mac Lean DF (1995) The validity of bitewing radiographs for dental identification of children. J Forensic Sci 40: 1055-1057.
- Wood RE, Kogon SL (2010) Dental radiology considerations in DVI incidents: A review. Forensic Sci Int 201: 27-32. [Crossref]
- Chiam SL (2014) A note on digital dental radiography in forensic odontology. J Forensic Dent Sci 6: 197-201. [Crossref]
- Wenzel A, Richards A, Heidmann J (2010) Matching simulated antemortem and postmortem dental radiographs from human skulls by dental students and experts: testing skills for patter recognition. J Forensic Odontostomatol 28:1:5-12
- Bajaj A (2005) Disaster victim identification: Tsunami. Br Dent J 198: 504-505. [Crossref]
- McCarney R, Warner J, Iliffe S, van Haselen R, Griffin M, et al. (2007) The Hawthorne Effect: a randomised, controlled trial. BMC Med Res Methodol 7: 30. [Crossref]
- Hogge JP, Messmer JM, Doan QN (1994) Radiographic identification of unknown human remains and interpreter experience level. J Forensic Sci 39: 373-377. [Crossref]