Inadequate support for placement of balloons or stents continues to be a problem in interventional cardiology. We read with interest the report on Mother-Daughter-Granddaughter Double Guide Liner Technique for Delivering Stents Past Multiple Extreme Angulations. The authors cleverly describe the use of a 6 French Guide Liner inside an 8 French Guide Liner to cross two difficult to cross saphenous vein graft lesions. We also read with interest the case report on how to perform distal anchoring technique by 6 French radial approach in complex coronary procedures. It reported utilizing an anchoring balloon technique passing the anchoring balloon in the distal portion of the vessel utilizing a 6 French radial approach.
If one cannot deliver stents to the target lesion, procedural success is impossible and failure can result in increased morbidity. We have been successful in utilizing a variant of the anchoring balloon technique in coronary and other complex interventions.
Inadequate support for placement of balloons or stents continues to be a problem in interventional cardiology. We read with interest the report on Mother-Daughter-Granddaughter Double Guide Liner Technique for Delivering Stents Past Multiple Extreme Angulations, by Finn, et al. [1]. The authors cleverly describe the use of a 6 French Guide Liner inside an 8 French Guide Liner to cross two difficult to cross saphenous vein graft lesions. We also read with interest the case report by Fiocca, et al., on How to perform distal anchoring technique by 6 French radial approach in complex coronary procedures [2]. They reported utilizing an anchoring balloon technique passing the anchoring balloon in the distal portion of the vessel utilizing a 6 French radial approach. If one cannot deliver stents to the target lesion, procedural success is impossible and failure can result in increased morbidity [3]. We have been successful in utilizing a variant of the anchoring balloon technique in coronary and other complex interventions with the Prodigy balloon [4] (Figures 4, 4a).
We describe a dedicated support device that can be utilized in coronary CTOs, complex saphenous vein graft and native coronary intervention as well as in PAD intervention [5]. The device is similar to a Guide Liner; however, the inner catheter theoretically is less likely to piston back as you aggressively attempt to pass balloon, atherectomy or stent devices through the daughter portion of the support catheter because the Daughter segment has a similar elastomeric balloon like the Prodigy that can be inflated from 1mm to 10mm in diameter (Figures 5, 5a). We describe this approach as an alternative to the distal anchoring technique described by Fiocca, et al., as well as the other daughter/granddaughter technique described by Finn, et al.
Guide Liner facilitated PCI is becoming increasingly common in clinical practice with Waterbury, et al., describing an 80% procedural success rate. It is also very useful in treating CTOs after the lesion has been crossed [2]. One of the issues with the Guide Liner is the possibility of dissection with deep engagement of the “Daughter” limb. Unlike, the Guide Liner, the inner portion of the CrossLock™ catheter that deeply engages the vessel has an elastomeric, very compliant balloon that can be dilated from 1mm to 10mm in diameter. We describe three cases where we utilized this device to perform complex coronary and peripheral interventions. In performing peripheral intervention, a support catheter allows for wire crossing, but then the support catheter must be removed. The CrossLock™ can remain in place and is the only device to allow placement of devices with enhanced support as well as centering to make crossing complex or CTO lesions theoretically easier.
A 71-year-old retired veteran presented with a chronic RCA CTO. He underwent RCA stenting 15 years ago, and had a previously placed AV sequential pacer. He underwent attempted CTO treatment via the right femoral artery with sheath placement of the left groin for possible Impella placement or retrograde approach. We used an 8 French JR4 guiding catheter and placed a .014 Miracle 3 wire through a FineCross through the CrossLock™ catheter. With the CrossLock™ balloon dilated and centering our position in the vessel, we quickly traversed the CTO with the wire and the FineCross. The Fielder XT was then used, but we were not able to advance further so we switched to a Whisper wire and advanced to the mid portion of the RCA. The FineCross was not able to be advanced, and we switched to the Caravel microcatheter. With further passage of the CrossLock™ and with the Caravel’s support, we successfully placed drug eluting stents to complete the procedure.
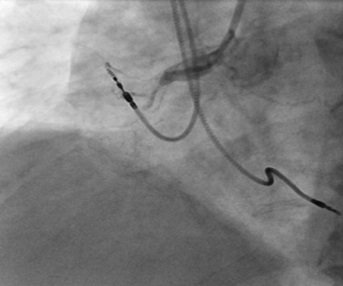
Figure 1. A right coronary angiogram performed with an 8 French JR4 guiding catheter.
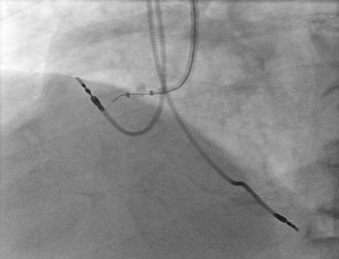
Figure 2. The CrossLock™ is in place at the origin of the RCA.
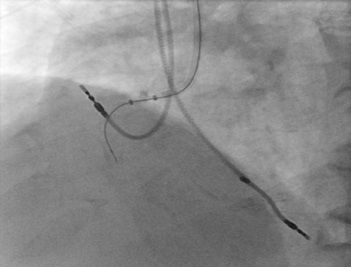
Figure 3. Utilizing the firm support with the CrossLock™ and with no pressure applied with a stiff guiding catheter, we were able to pass into the CTO. Note the miracle 3 wire is inside a FineCross catheter.
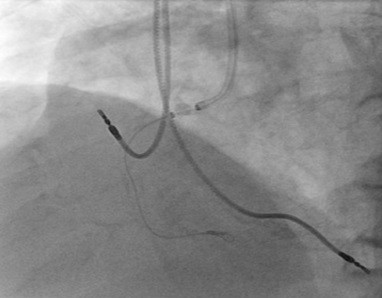
Figure 4. The caravel catheter makes it possible to pass further across the entire vessel.

Figure 4a. The Prodigy™ catheter.
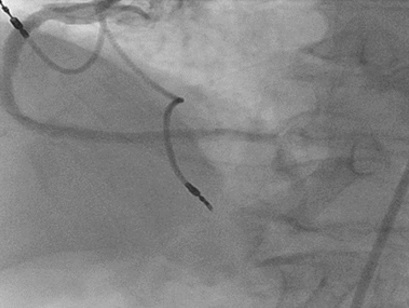
Figure 5. Final result after PTCA and drug eluting balloon placement supported by the CrossLock™.

Figure 5a. The CrossLock™ catheter. This is what the device looks like with the balloon inflated. The balloon can be inflated from 1 mm to 8 mm.
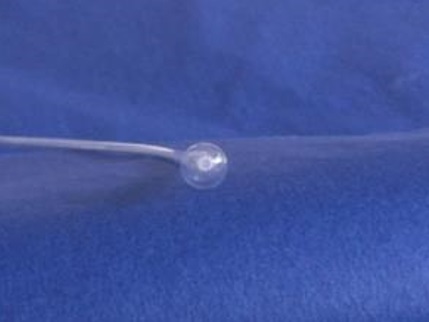
Figure 5b. The CrossLock™ seen at the tip.
A 60-year-old presents with RCA ISR. He is status post CABG in 1997 with both SVG to RCA and circumflex occluded and a patent left internal mammary to the LAD. On 9/14, he underwent PTCA for 2 stent ISR lesions. During previous intervention, it was noted that there was difficulty with guide support and a very stiff Amplatz guide needed to be used to pass the balloon catheters across the lesions. He now presents with angina with minimal activity and an outside angiogram revealed recurrent ISR and an EF of 40%. An 8 French JR4 guide was used and the CrossLock™ was inserted over an .014 Whisper wire and FineCross. The inflation of the CrossLock™ aided the passing of the wire, FineCross and subsequent .9mm Laser over the lesions. Following this, a 3.5mm x 8mm Alpine stent was placed at the distal ISR site and a 3.5mm x 12mm placed at the proximal lesion. The vessel was widely patent following treatment.
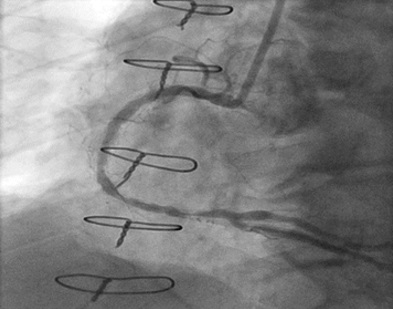
Figure 6. A JR4 8 French guide is at the origin of the right coronary artery. Angiography shows two focal instent restenotic lesions.
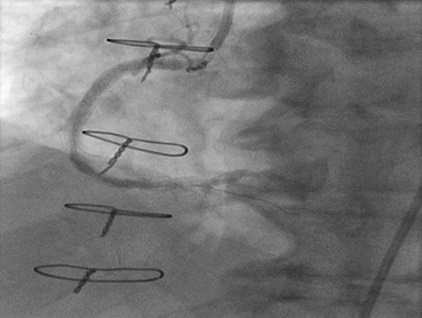
Figure 7. The CrossLock™ is in place at the origin of the vessel allowing placement of the .9mm Laser (not shown).
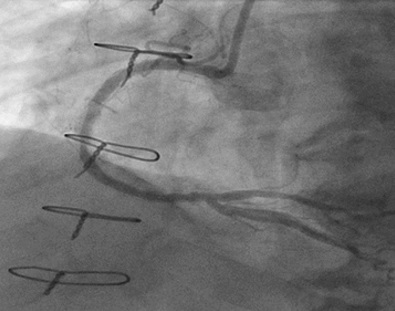
Figure 8. Final angiogram after laser PTCA and drug eluting stenting of the two lesions with the CrossLock™ now removed.
A 70-year-old gentleman with an extensive history of tobacco abuse and a non-ischemic cardiomyopathy presents with left leg claudication for the last 8 years. His resting ABIs are right 1.00, left .80. A 6F Ansel (Cook Medical) was selectively engaged into the common femoral artery and in spite of the fact that it was difficult to delineate the origin of the SFA, we passed the .014 Command wire (Abbott Vascular, Abbott Park, Illinois) with the CrossLock™ balloon catheter. The FrontRunner™ was passed through the Rx port of the CrossLock™ and with the wire pulled back and the CrossLock™ balloon inflated, we were able to pass the FrontRunner™ across the total occlusion. This was followed by balloon angioplasty and then multiple drug eluting balloons (Lutonix, Bard Peripheral, Tempe, Arizona). Following this, there was excellent patency and runoff.
The new Caravel catheter has an extremely low profile (1.9 French) and is able to traverse difficult lesions to aid wire placement. We also know from our work with the CrossLock™ centering device, in multiple coronary and peripheral interventions, that multiple devices like the Caravel catheter can fit through the lumen without any difficulty with the centering feature aiding in intraluminal delivery. Those devices include the Crosser, Front Runner, 9 Laser, True Path, Viance and the CrossBoss. Until the development of the CrossLock™, peripheral intervention support catheters could only be utilized for lesion crossing with the wire. With the Cross Lock™ device, one can be centered in the lumen for wire crossing and with the compliant balloon still in place then advance a dedicated crossing device, ablative device, balloons, or stents.
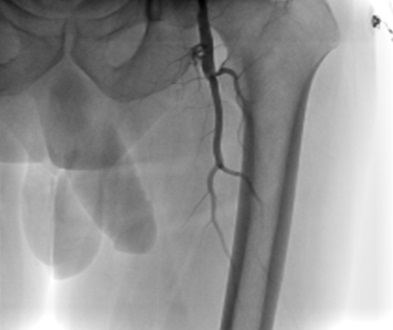
Figure 9. Total occlusion of the SFA.

Figure 10. Note the absence of a true origin treatment zone.
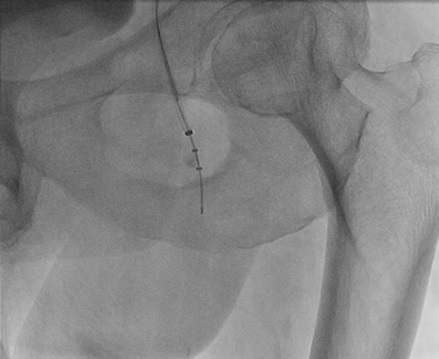
Figure 11. The CrossLock™ has been passed over a .014 wire and the FrontRunner™ is also in place. Note the balloon on the CrossLock™ is inflated centering the lumen for passage of the FrontRunner™. It subtends the CTO in real time.

Figure 12. The CrossLock™ has been deflated, and it is advanced over the FrontRunner™.

Figure 13. The CrossLock™ and Front Runner™ were removed and a Glide catheter was passed over the .014 wire and an .035 wire is now passed in an intraluminal position.
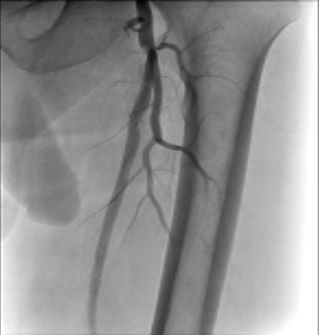
Figure 14. Final angiogram showing 3 vessel runoffs.
The CrossLockTM device is another option for interventional support that may be useful, not only in saphenous vein graft as well as native coronary interventions. It may also be effective in peripheral and coronary CTOs.
- Finn MT, Green P, Nicholson W, Kalra S, Kandzari DE, et al. (2016) Mother-Daughter-Granddaughter Double GuideLiner Technique for Delivering Stents Past Multiple Extreme Angulations. Circ Cardiovasc Interv 9: e003961. [Crossref]
- Fiocca L, Bernelli C, SIrbu V, Musumeci G, Guagliumi G, et al. (2016) How to perform distal anchoring technique by 6 French radial approach in complex coronary procedures. Cardiovasc Revasc Med : 339-343. [Crossref]
- Cantor WJ, Lazzam C, Cohen EA, Bowman KA, Dolman S, et al. (1998) Failed coronary stent deployment. Am Heart J 136: 1088-1095. [Crossref]
- Moualla SK, Khan S, Heuser RR (2014) Anchoring improved: introduction of a new over-the-wire support balloon. J Invasive Cardiol 26: E130-132. [Crossref]
- Heuser RR, Zang K, Mollen AJ (2016) A Step Forward: The Use of the CrossLock Catheter in a Patient With Critical Limb Ischemia and a Popliteal Occlusion. J Invasive Cardiol 28: E13-16. [Crossref]