Cardioembolic stroke is largely preventable, warranting efforts at primary prevention for major risk cardioembolic sources [1]. Ultrasound diagnostic techniques such as echocardiography have allowed clinicians to better characterize well-established sources of embolism and to discover other potential etiologies of cardioembolic stroke [2]. The more common high risk cardioembolic conditions are atrial fibrillation, recent myocardial infarction, mechanical prosthetic valve, dilated myocardiopathy, and mitral rheumatic stenosis. Cardiac emboli arising from the cardiac chambers are often large and hence especially likely to cause severe stroke, disability and death [3].
Detecting athletes with underlying heart disease is a great challenge for sports cardiology medicine. The goals of sports pre-participation screening are to prevent sudden death and other cardiovascular accidents in athletes. Herewith the author describes the history of an otherwise healthy 60-year-old amateur rider who came to our sports cardiology medicine center for sports pre-participation screening. His family history was unremarkable and physical examination was normal. He claimed he felt fit and that he was taking regular physical activity by cycling. His old ECG of 2014 was normal (Figure 1); the last ECG of 2015 (Figure 2) was abnormal for findings of recent anterior myocardial infarction. A subsequent echocardiogram through classical and magnified apical 4 chamber view showed left ventricular apical akinesis with small apical thrombus (Figure 3) which protrudes into the cavity and demonstrates mobility in real-time imaging (Videos 1 & 2). The athlete was admitted to cath lab for revascularization procedure and anticoagulation therapy was started. The risk of cardioembolic stroke was very high. Trans-thoracic echocardiography (TTE) is usually the initial cardiac imaging modality, and reliably detects left ventricular wall motion abnormalities, and left ventricular thrombus. Nowadays, its use in sports cardiology medicine is mandatory to detect underlying and dangerous heart disease such as myocardial infarction complicated with LV thrombus in asymptomatic athletes [4].
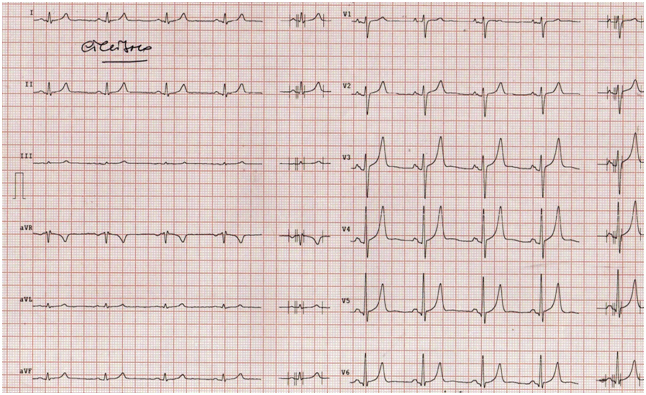
Figure 1: Normal ECG of 2014.
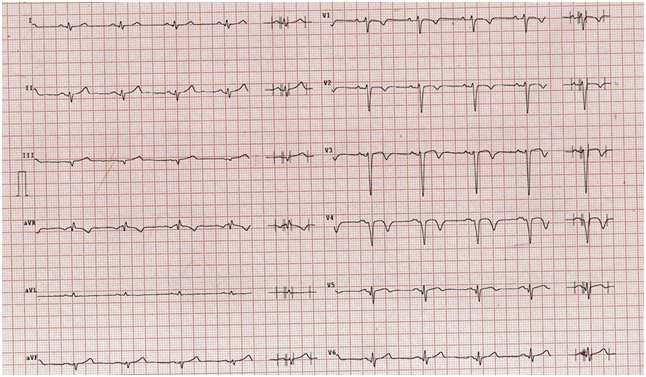
Figure 2: Abnormal ECG of 2105 with findings of anterior myocardial infarction.
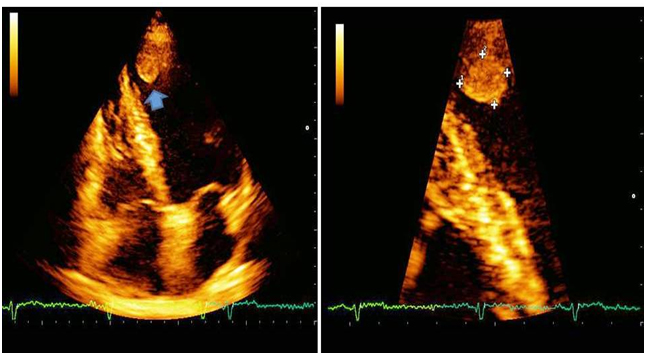
Figure 3: Echocardiographic findings of left ventricular apical thrombus (see arrow and magnified imaging) by apical 4 chamber view.
Disclosures
None
References
Hart RG, Albers G, Koudstaal P (1998)Cardioembolic stroke. Ginsberg M, Bogousslavsly J, eds. Cerebrovascular Disease: Pathophysiology, Diagnosis and Management. Blackwell Science1998: 1392-429.
Wessler BS, Kent DM (2015) Controversies in cardioembolic stroke. Curr Treat Options Cardiovasc Med 17:358.[Crossref]
Arboix A, Alió J (2010)Cardioembolic Stroke: Clinical Features, Specific Cardiac Disorders and Prognosis. Curr Cardiol Rev6:150-161.[Crossref]
BolognesiM (2016). An otherwise healthy athlete at high risk of cardioembolic stroke.Gen Int Med ClinInnov1: doi:10.15761/GIMCI.1000105
Corresponding author
Massimo Bolognesi, MD
Department of Internal General Medicine, Sports Cardiology Medicine Center, AziendaUnità Sanitaria Locale della Romagna, Via Ungaretti, 494 , 47521 Cesena, Italy, Tel: +390547645074
Video 1 and 2:LV apical akinesis with small apical thrombus which protrudes into the cavity and demonstrates mobility by classical and magnified apical 4 chamber view.
Figure 1: Normal ECG of 2014.
Figure 2: Abnormal ECG of 2105 with findings of anterior myocardial infarction.
Figure 3: Echocardiographic findings of left ventricular apical thrombus (see arrow and magnified imaging) by apical 4 chamber view.