Internal maxillary artery injury is life threatening injury. It needs immediate intervention to save victim life. This case is very unusual because the intervention was not definite but was saving the patient life. This went for all most two months. The surgical challenges to have definite treatment for the internal maxillary artery injury needs very well experience Oral and Maxillofacial or head and neck surgeon with very well-trained team. Bullet is distractive mechanism for both hard and soft tissues
bullet, injury, internal maxillary artery, external carotid artery, common carotid artery, severe
The internal maxillary artery injury is very hard to manage in peace how about if that happen in war. The complexity of the anatomical location of the internal maxillary artery and the surrounding vital structures makes it very challenging to manage. This case is very unique because in the field where the fighting is going the victim was saved and evacuated back to the field medical unit where there controlled the hemorrhage then evacuated the Maarb Hospital in Yemen that time no active bleeding after two weeks had severe bleeding. Patient got blood transfusion and transferred to Sharrora Saudi Arabia medical team closed the intraoral wound then three weeks later had episode of severe bleeding got blood transfusion and contacted Alqathi Specialist Hospital in Najran transfer patient to it. [1-3].
This case from the Yemeni soldier fighting against the Huthi faction. 20 years old male soldier sustained bullet injury. The bullet interred medial superior to the left malar via the maxillary sinus more posterior inferior into the mandible from superior inferior lateral which is all the hard and soft tissues destroyed as it showed in the CT scan (Figure 1) which is done in Alqathi Specialist Hospital in Najran patient was evaluated radiographically and clinically the finding were left medial superior malar region fistula with sorma like discharge intraoral defect in the maxilla telescoped and comminuted left mandible, shifted the lower jaw to the left. The patient booked for exploration surgery and repair of the comminute bony fragments that after more than two months of injury. Under general anesthesia nasal intubation patient is prepped and draped for the procedures. Internal maxillary mandibular fixation (IMF) with arch bars and wires is done. Extra oral approach is proceeded left submandible incision then layer by layer dissection was performed and exposed the mandible and removed the callus reduce the fractured bones then secured plates and screws and closed the wound in layer [4-8]. The IMF released and checked the occlusion and explored the gunshot wound on the left maxillary region during the procedure from big defect in maxilla bleeding but was not significant controlled with surge cell and gel foam and buccal rotating flap and closed patient then the left facial bullet fistula removed and closed (Figure 2). The endotracheal tube is removed and patient rolled to the post anesthesia unit in stable condition thereafter to the normal floor then back to the center in Sharrorah three weeks later very frank arterial bleed from the left maxillary defect send back to Alqathi Specialist Hospital in Najran local majors used and stopped the bleeding then two week the visiting surgeon returned to Alqathi Specialist Hospital the morning of arrival patient bled due to limited resources including lack of the ability to do angiography and embolization of injured left internal maxillary artery. The patient was taken to the operating room incision made and layer by layer dissection is done exposed the common carotid fallow it until the external carotid artery then ligated and closed the wound layer by layer (Figure 3) then went back the regular floor. In case of bleeding that is difficult to control ligation of external carotid artery is necessary. Since then the patient is function normally as appear picture (Figure 2).
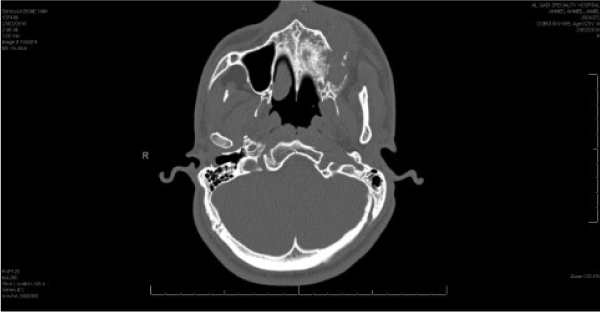
Figure 1. CT scan of bullet interred medial superior to the left malar.

Figure 2. Left facial bullet fistula removed and closed.

Figure 3. Operating room incision made and layer by layer dissection.
Now days in active war an injury can be debilitating, because the power and the velocity of the projectiles (bullet, missile and shrapnel) are used in the battle field. Any projectile entry in the head and neck region can be very distractive to vital such as nerves, blood vessels, muscles and bones. Internal maxillary artery injury is life threatening injury. Therefor immediate tension for these victims with is most however in the battle field very difficult. So most of battle field injuries either death or permanent disability [9-12]. Management of internal maxillary artery injury is not like any blood vessels injury due to the anatomical complexity. This case had injury with high velocity bullet is greater than 2000 feet per second. Victim of high velocity ballistic injury is rarely survived the injury. Nevertheless, internal maxillary artery with result pseudoaneurysms secondary to gunshot in jury have been sited and managed using endovascular methods. Bullet, missile and shrapnel to the head and neck region can be life threatening situation due to the vital structures located in this exposed region. Various methods to address the internal maxillary artery bleeding have been described. Yeo and et al, outlined direct pressure, packing and topical hemostatic agents as the first steps for attempting hemostasis. Failure of these measure may prompt surgical ligation of origin of the maxillary artery. The other option is selective angioembolisation or an ipsilateral neck incision and placement of an external carotid artery sling followed by direct surgical ligation of the maxillary artery. Evidence from a systemic review by Khanna and coworkers supports the modality of transcatheter arterial embolization (TAE) hemostasis of life-threatening hemorrhage in maxillofacial surgery [13-15]. TAE is becoming the gold standard because it obviates the need for surgical incision and allows flexibility in reaching sites inaccessible to surgical ligation. Also, can be used to detect arteriovenous malformation or false aneurysms. However, in the battle field or not well-prepared hospital for such complex cases pressure, packing, and surgical intervention with very well experienced surgeon still the way to save life. The internal maxillary artery injury from bullet, missile or shrapnel always has dangerous consequences.
Trauma management in the battle field and under prepared facility can be very challenging. Therefore quick and organized thinking with experience would reduce the mortality rate in these trauma victims. This case unique because almost two months with just minimal intervention due many factors, battle field after evacuation lack of materials and expertise until it transferred to Alqathi Specialist Hospital. The surgical option in such situation is the best option.
Mr. Agial Mohammad, all OR Nurses and Technicians, Medical Director, CEO Mr. Randal, Mr. Ali Algathi all administration for doing everything to serve the war victims.
- Orbay H, Kerem M, Unlu RE, Comert A, Tuccar E, et al. (2007) Maxillary artery anatomical landmarks and relationship with mandibular subcondyle. Plast Reconstr Surg 120: 1865-1870. [Crossref]
- Morton AL, Khan A (1991) Internal maxillary artery variability in the pterygopalatine fossa. Otolaryngol Head Neck Surg 104: 204-209. [Crossref]
- Choi EC, Choi Ys, KimCH, Kim K, Kim KS, et al. (2004) Surgical outcome of radical maxillectomy in advanced maxillary sinus cancer. Yonei Med J 45: 621-628. [Crossref]
- Yeo Ms, Goh TL, Nallatamby V, Cheong EC, Lim TC (2012) Maxillary artery injury associated with subcondylar mandible fracture: a novel treatment algorthim. Craniomaxillofac Trauma Reconstr 5: 83-88. [Crossref]
- Kaufman Y, Cole P, Hollier LH Jr (2009) Facial gunshot wounds: trends in management. Craniomaxillofac Trauma Reconstr 2: 85-90. [Crossref]
- Khanna S, Dagum AB (2012) A critical review of the literature and an evidence-based approach for life-threatening hemorrhage in maxillofacial surgery. Ann Plast Surg 69: 474-478. [Crossref]
- dos santos Pereira R, de Souza Guiaraes VC, Timoteo CA, Homsi N, da Rocha HV Jr, et al. (2014) Internal maxillary artery pseudoaneurysm subsequent gunshot wound in teenager. J craniofac Surg 25: 1125-1126. [Crossref]
- Wang CP, Yang TL, Ko JY, Lou PJ (2007) Ligation of the internal maxillary artery to reduce intraoperative bleeding during total maxillectomy. Larygoscope 117: 1978-1981. [Crossref]
- Choi J, Park HS (2003) The clinical anatomy of the maxillary artery in the pterygopalatine fossa. J Oral Maxillofac Surg 61: 72-78. [Crossref]
- Pothier DD, Mackeith S, Youngs R (2005) Sphenopalatine artery ligation: technical note. J Laryngol Otol 119: 810-812. [Crossref]
- Lanigan DT, Hey J, West RA (1991) Hemorrhage following mandibular osteotomies: a report of 21 cases. J Oral Maxillofac Surg 49: 713-724. [Crossref]
- Roberti F, Boari N, Mortini P, Caputy AJ (2007) The pterygopalatine fossa: an anatomic report. J Craniofac Surg 18: 586-590. [Crossref]
- Lasker GW, Opdyke DL, Miller H (1951) The position of the internal maxillary artery and its questionable relation to the cephalic index. Anat Rec 109: 119-126. [Crossref]
- Krishnan DG, Marashi A, Malik A (2004) pseudoaneurysm of internal maxillary artery secondary to gunshot wound managed by endovascular technique. J oral maxillofac Surg 62: 500-502. [Crossref]
- Holt GR, Kostohryz G Jr (1983) Wound ballistics of gunshot injuries to the head and neck. Arch Otolaryngol 109: 313-318. [Crossref]