Abstract
Macular involvement in glaucoma has long been considered a late manifestation of the disease. However, increasing evidence suggests that damage to the macular region may occur early, particularly in normal-tension glaucoma, leading to disproportionate impairment of central vision. We report the case of a 39-year-old woman who presented with progressive reduction in distance visual acuity and reading difficulty. Ophthalmological examination revealed normal intraocular pressure, enlarged optic disc cupping with temporal pallor, and no clinically visible macular abnormality. Automated perimetry demonstrated a juxtafoveal scotoma involving fixation despite mildly altered global indices. Optical coherence tomography showed marked thinning of the temporal retinal nerve fiber layer and diffuse loss of the macular ganglion cell complex. In the absence of cataract or primary macular pathology, a diagnosis of early-stage normal-tension glaucoma with significant macular involvement was established. Treatment with a topical prostaglandin analog led to partial improvement in corrected distance visual acuity over a two-year follow-up, while structural and functional defects remained stable. This case emphasizes that macular damage may occur early in glaucoma and highlights the importance of systematic macular evaluation using central visual field testing and macular OCT, even in patients classified as having early disease.
Keywords
glaucoma, normal-tension glaucoma, macular involvement, ganglion cell complex, optical coherence tomography, central visual field
Introduction
Glaucoma is traditionally described as a disease primarily affecting peripheral vision, with central visual function preserved until advanced stages. As a result, early loss of visual acuity in glaucoma patients is often attributed to coexisting ocular conditions such as cataract or macular disease. Recent studies, however, have demonstrated that the macular region containing a high density of retinal ganglion cells may be affected early in the disease course, particularly in normal-tension glaucoma. We report a case illustrating early macular involvement responsible for significant central visual impairment despite mild global visual field loss.
Case presentation
A 39-year-old woman with no known ophthalmological history presented in 2017 to a private ophthalmology clinic “AFIA clinic” in Lomé, Togo, complaining of progressive deterioration of distance vision associated with increasing difficulty in reading over several months. She reported no ocular pain or acute visual symptoms.
Uncorrected distance visual acuity was 4/10 in the right eye and 3/10 in the left eye. Near visual acuity was Parinaud 8 bilaterally. After optical correction, distance visual acuity improved to 5/10 in both eyes and near visual acuity to Parinaud 3. Slit-lamp examination of the anterior segment was normal, with no evidence of cataract or media opacity. Intraocular pressure measured by applanation tonometry was 12 mmHg in both eyes.
Fundus examination revealed bilateral enlargement of optic disc cupping, with a cup-to-disc ratio of approximately 0.6 and associated temporal pallor. No clinically visible abnormality of the macula was observed.
Central corneal thickness was markedly reduced, measuring 420 µm in the right eye and 434 µm in the left eye, suggesting an underestimation of true intraocular pressure values.
Automated visual field testing using an Octopus 300Series perimeter (Haag-Streit) revealed a juxtafoveal scotoma involving the fixation point in the right eye (Figure 1) and the left eye (Figure 2), with a mean deviation less than 6 dB, consistent with early-stage glaucoma. Despite relatively preserved global indices, the focal and central nature of the defect explained the patient’s significant functional complaints.
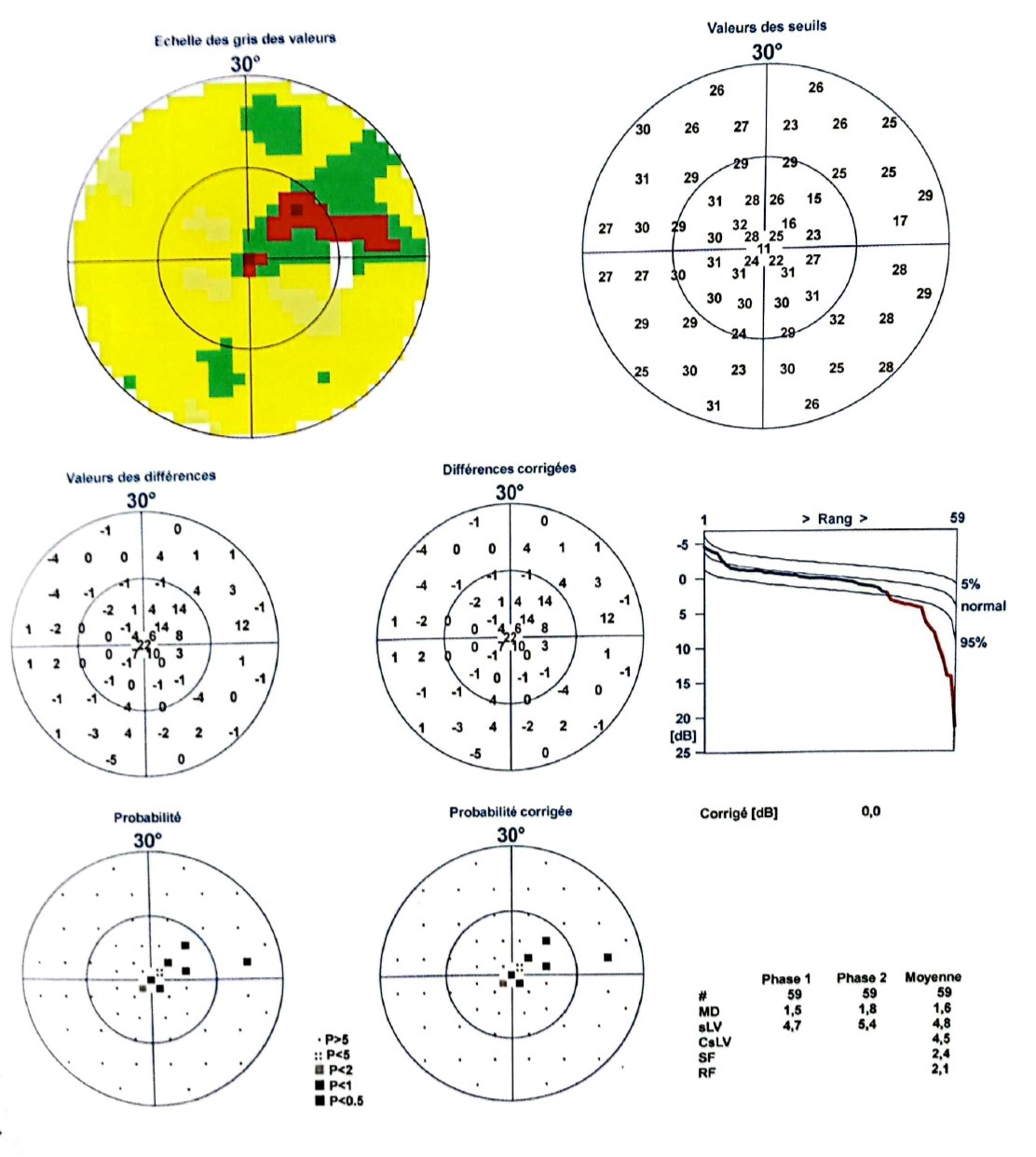
Figure 1. Juxtafoveal scotoma reaching the fixation point on the Right Visual Field Testing
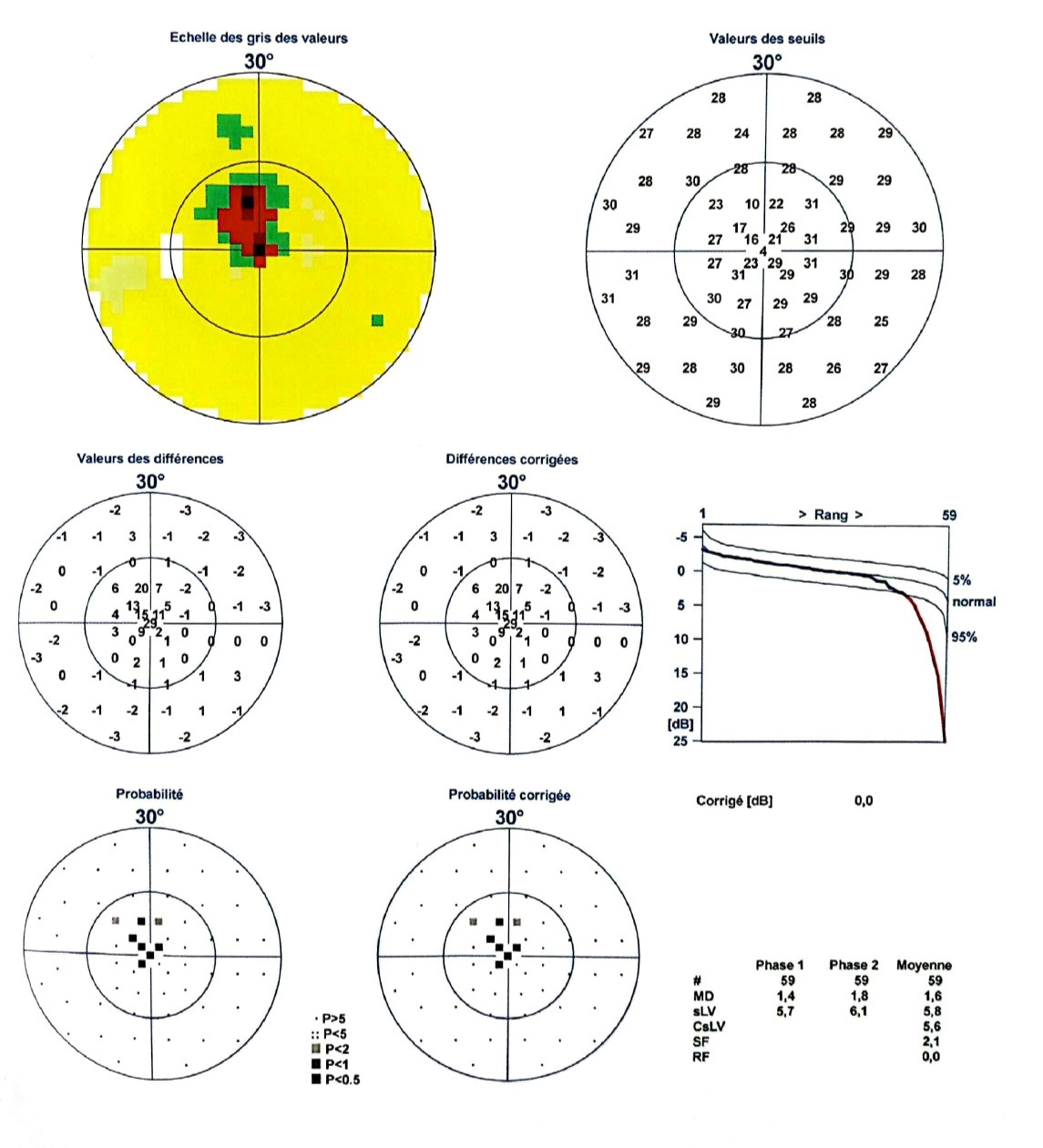
Figure 2. Juxtafoveal scotoma reaching the fixation point on the Left Visual Field Testing
Optical coherence tomography (3D OCT-2000, Topcon) of the optic nerve head demonstrated marked sectoral thinning of the temporal retinal nerve fiber layer, with vertical cup-to-disc ratios of 0.76 in the right eye and 0.70 in the left eye (Figure 3). Ganglion cell complex OCT revealed diffuse thinning of the ganglion cell complex in the parafoveal region in right eye (Figure 4) and in the left eye (Figure 5).
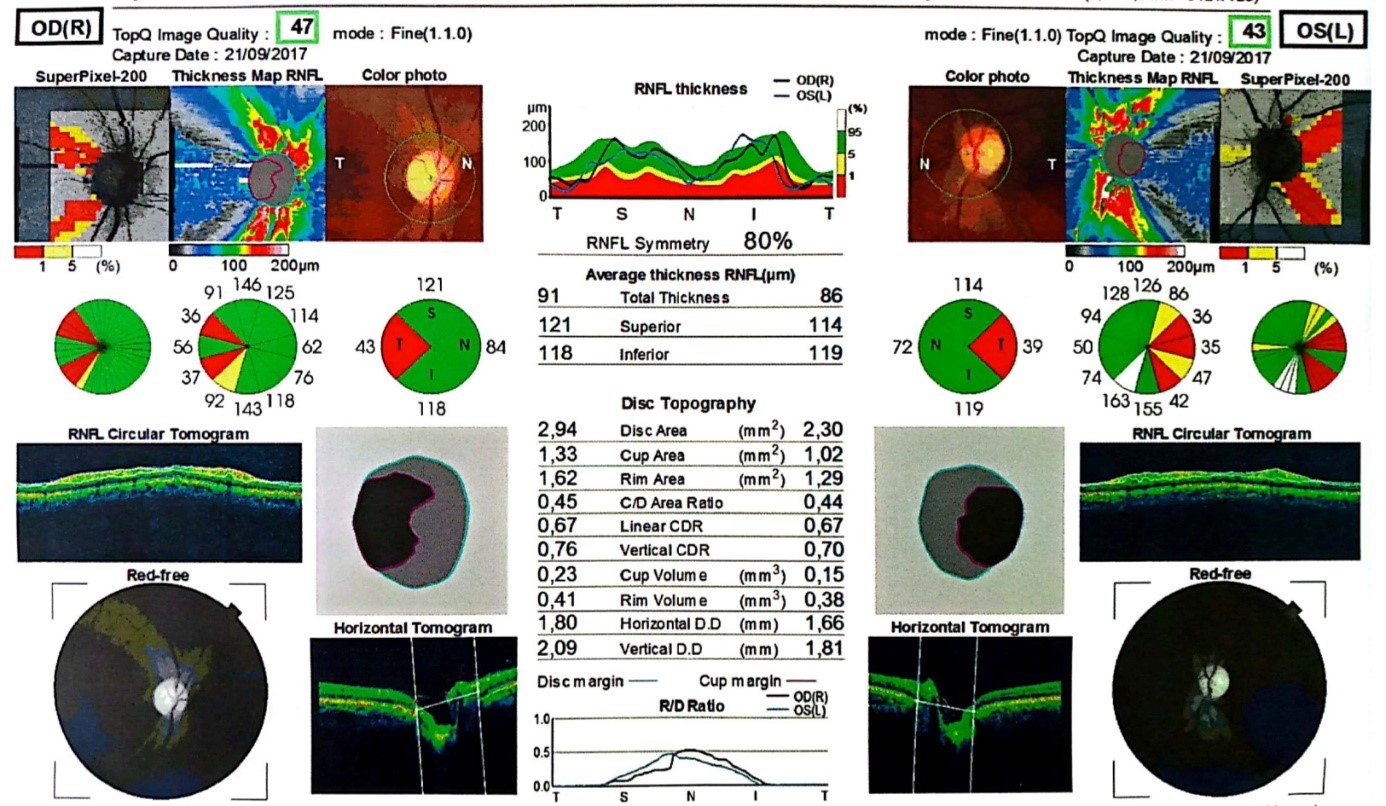
Figure 3. Thinning of the retinal nerve fiber layer (RNFL) in the temporal sector in the both eyes on Optic Nerve Head OCT
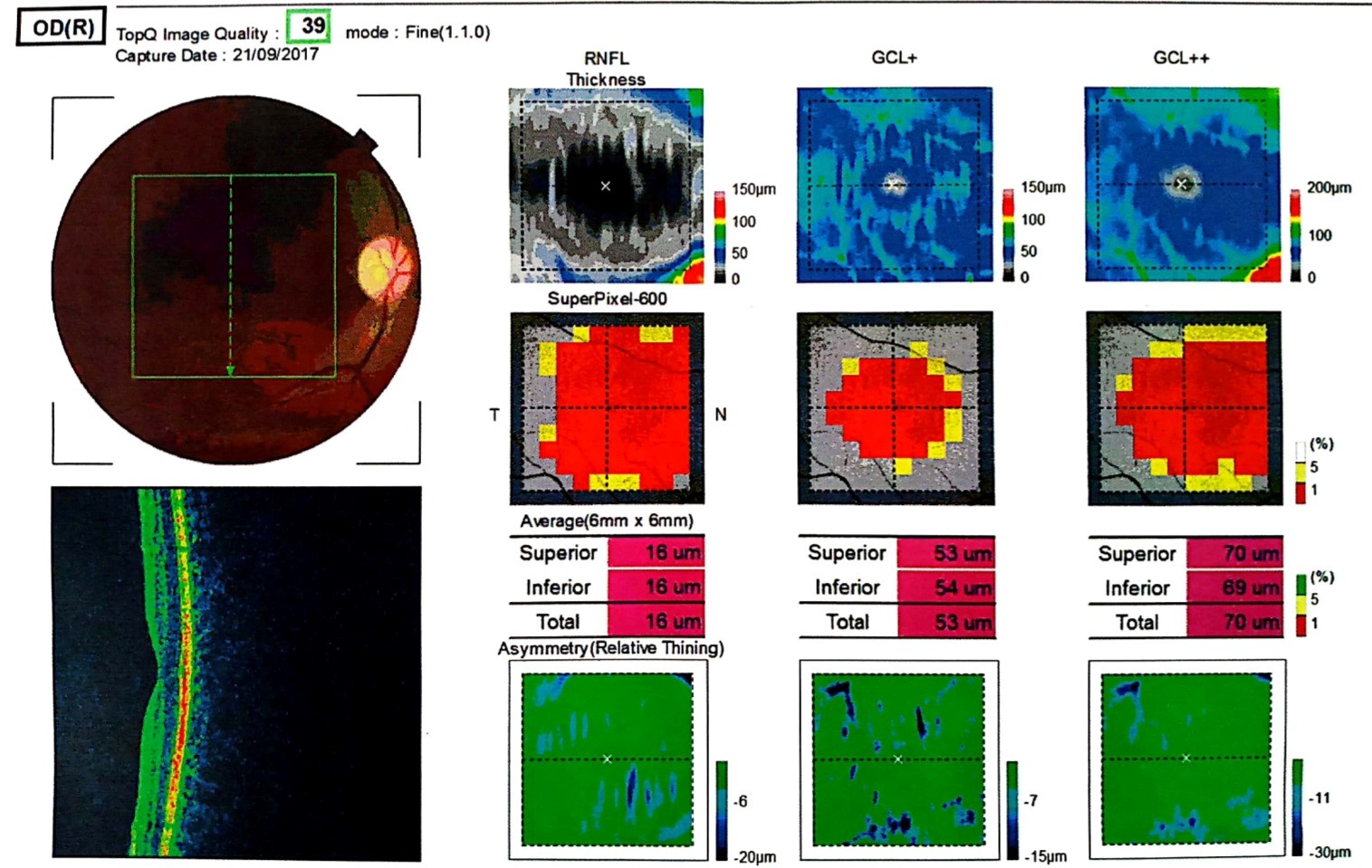
Figure 4. Diffuse thinning of the ganglion cell complex in the parafoveal region in right eye on the Ganglion cell complex OCT
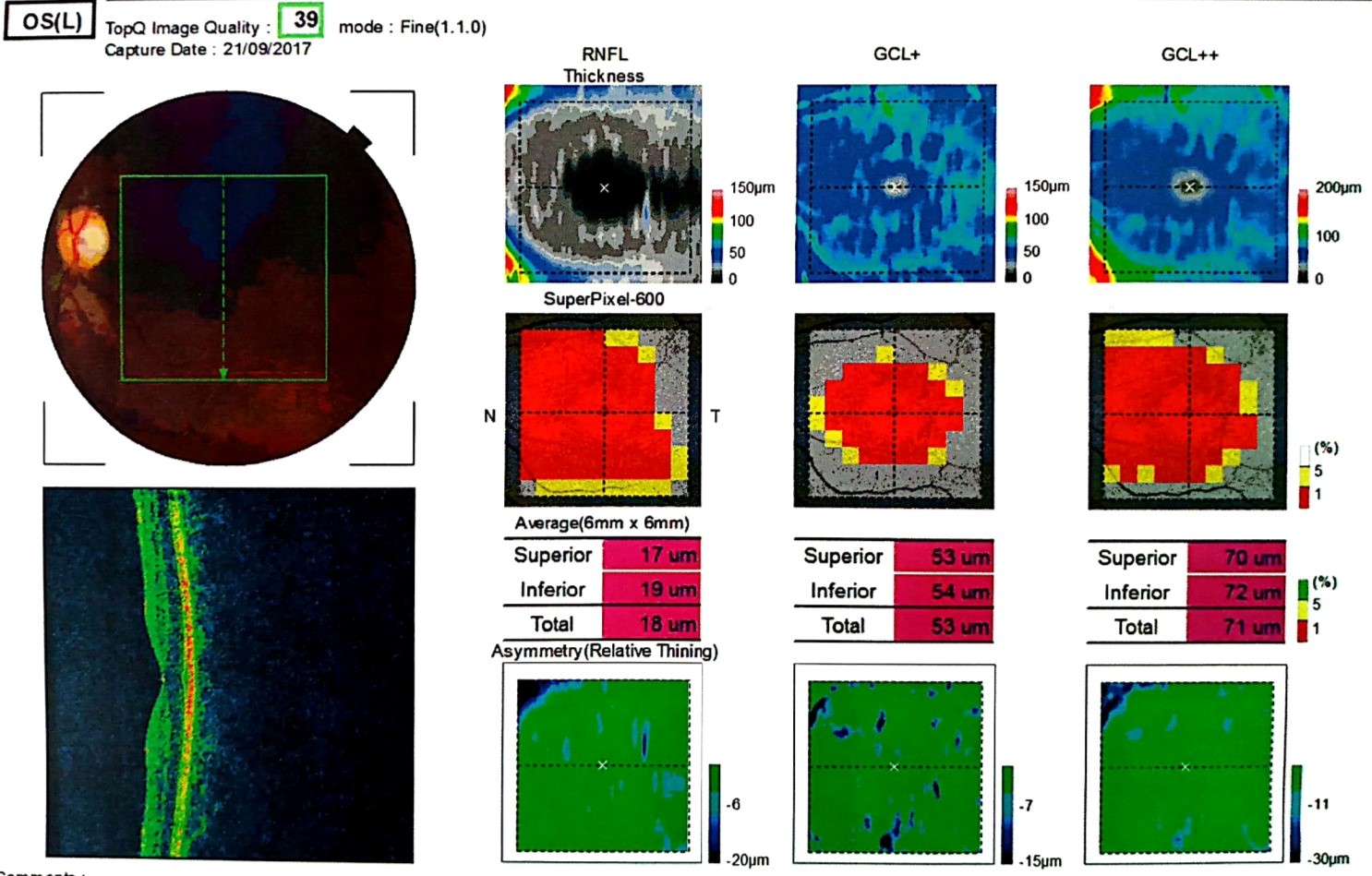
Figure 5. Diffuse thinning of the ganglion cell complex in the parafoveal region in left eye on the Ganglion cell complex OCT
Timeline
• Several months before consultation: Progressive decrease in distance vision and reading difficulty
• Initial visit (2017): Normal intraocular pressure, enlarged optic disc cupping, central visual field defect
• Diagnostic work-up: OCT showing temporal RNFL thinning and diffuse macular GCC loss
• Treatment initiation: Topical bimatoprost once daily
• Follow-up at 2 years: Improved corrected distance visual acuity, stable visual field and OCT findings
Diagnostic assessment and therapeutic intervention
In the absence of cataract, media opacity, or primary macular disease, the combination of central visual field loss, macular ganglion cell complex thinning, temporal retinal nerve fiber layer loss, and thin corneas supported the diagnosis of early-stage normal-tension glaucoma with significant macular involvement. Differential diagnoses, including optic neuropathies and macular dystrophies, were considered unlikely based on clinical and imaging findings.
Treatment with topical bimatoprost, one drop nightly in both eyes, was initiated to further lower intraocular pressure and reduce the risk of disease progression.
Follow-up and outcomes
After two years of treatment and follow-up, corrected distance visual acuity improved from 5/10 to 7/10 in both eyes. Near visual acuity, visual field defects, and optic disc appearance remained stable. No disease progression was observed on OCT imaging during follow-up.
Discussion
This case illustrates a now well-established but still underestimated concept in clinical practice: macular involvement can occur at an early stage of glaucoma and be responsible for major functional impairment, despite relatively preserved global visual field indices [1]. The perifoveal ganglion cell layer contains the highest concentration of retinal ganglion cells, whereas the fovea itself is devoid of ganglion cells but rich in cones. Because ganglion cells are displaced approximately 500 µm from the photoreceptors, the perifoveal ganglion cell layer plays a key role in central vision. Diffuse damage to this layer explains central vision loss and difficulties with light adaptation [2].
Historically, glaucoma was considered a disease initially affecting peripheral vision, with central vision compromised only at advanced stages. This concept led clinicians to attribute any decrease in visual acuity in early glaucoma to associated conditions such as cataract or maculopathies. However, several studies have challenged this paradigm by demonstrating that the macula is frequently involved, sometimes early, in glaucoma [1–5]. Hood, et al. [3] showed that glaucomatous damage preferentially affects the macular ganglion cell complex (GCC) and that standard 24-2 perimetric strategies often underestimate central defects. They recommend systematic use of 10-2 visual field testing for a more detailed analysis of the macular region, particularly when macular OCT shows GCC damage [1,5].
Anatomically, the macula contains more than 50% of retinal ganglion cells, mainly concentrated in the perifoveal ganglion cell layer. Although the fovea itself lacks ganglion cells, their displacement relative to photoreceptors explains why diffuse damage to the perifoveal ganglion cell layer can result in significant central vision impairment, as observed in our patient [1,2,6]. Several studies have demonstrated a close correlation between macular GCC thinning on OCT and the presence of paracentral or juxtafoveolar scotomas, sometimes involving the fixation point [3,5,7,8]. Blumberg et al. further showed that these central defects are associated with a significant reduction in quality of life, particularly affecting reading and light adaptation, justifying more aggressive therapeutic management in patients with macular involvement, even at an early stage [4]. More recent OCT angiography data suggest that structural damage to the macular GCC is associated with reduced macular vessel density, supporting the hypothesis of a structure–function–vascular coupling in early glaucoma [9].
This case confirms that glaucoma classification based solely on mean deviation can be misleading when the defect is highly localized and central. A multimodal approach combining central visual field testing, ganglion cell complex OCT, and optic disc OCT is essential for accurate functional assessment and therapeutic decision-making.
Conclusion
Macular damage may occur early in glaucoma and lead to substantial impairment of central vision, particularly in normal-tension glaucoma. Systematic evaluation of the macular region using macular OCT and central visual field testing is essential, even in early-stage disease, to ensure accurate diagnosis and appropriate management aimed at preserving central visual function.
Conflicts of interest
The authors declare no competing interests.
Ethics statement
Written informed consent was obtained from the patient for publication of this case report and associated images, in accordance with CARE guidelines.
References
- Hood DC, Raza AS, de Moraes CG, Liebmann JM, Ritch R (2013) Glaucomatous damage of the macula. Prog Retin Eye Res 32: 1-21. [Crossref]
- Zeitoun M (2013) Clinical forms of macular glaucoma assessed by optical coherence tomography. J Fr Ophtalmol 36: 299-309.
- Hood DC, Slobodnick A, Raza AS, de Moraes CG, Teng CC, et al. (2014) Early glaucoma involves both deep local, and shallow widespread, retinal nerve fiber damage of the macular region. Invest Ophthalmol Vis Scie 55: 632-649. [Crossref]
- Blumberg DM, De Moraes CG, Prager AJ, Yu Q, Al-Aswad L, et al. (2017) Association between undetected 10-2 visual field damage and vision-related quality of life in patients with glaucoma. JAMA Ophthalmol 135: 742-747. [Crossref]
- Traynis I, De Moraes CG, Raza AS, Liebmann JM, Ritch R, et al. (2014) Prevalence and nature of early glaucomatous defects in the central 10 of the visual field. JAMA Ophthalmol 132: 291-297. [Crossref]
- Santos MAK, Vonor K, Maneh N (2024) Clinical profile of patients with macular glaucomatous involvement at the perimetric stage in Lomé. J Fr Ophtalmol 47: 103970.
- Park SC, De Moraes CG, Teng CC (2011) Macular ganglion cell-inner plexiform layer thickness in glaucoma. Ophthalmol 118: 1031-1037.
- Hou H, Moghimi S, Zangwill LM (2020) Inter-eye asymmetry of macular ganglion cell complex thickness in early glaucoma. Ophthalmol 127: 1133-1144.
- Yarmohammadi A, Zangwill LM, Diniz-Filho A, Suh MH, Manalastas PI, et al. (2016) Optical coherence tomography angiography vessel density in healthy, glaucoma suspect, and glaucoma eyes. Invest Ophthalmol Vis Sci 57: OCT451-OCT459. [Crossref]