Abstract
Intracerebral hemorrhage (ICH) is a common cause of stroke, however, hemorrhage due to rupture of lenticulostriate aneurysms is a rare entity with only approximately 112 cases reported in the literature to date. We are presenting a case of basal ganglia bleed in a known case of hypertensive and diabetic with RT- PCR positive status for SARS CoV-2 whose CT angiography showed a “spot sign” in the right basal ganglia suggestive of Charcot aneurysm. Radiological imaging demonstration of structural cause of vasculopathy leading to ICH in a young patient even with risk factors like hypertension and diabetes mellitus is imperative for guiding further treatment. In the present scenario, there is also a recorded increased association of cerebrovascular accident (CVA) with covid infection. Both ICH bleeds associated with a covid patient and Charcot aneurysm is not quite well-understood entities. Through this case report we emphasize the role of radiological imaging using CT angiography in ICH due to ruptured Charcot aneurysm. In our case the possibility of covid being an aggravating factor is ruled out based on the time of presentation and location of the bleed.
Key words
Charcot bouchard microaneurysm, CT angiography, lenticulostriate, SARS-Cov-2, stroke
Introduction
Intracerebral hemorrhage is a common cause of stroke, however, hemorrhage due to rupture of lenticulostriate aneurysms is very rare with only 112 cases reported to date [1]. In the previous studies reported to date, it has been associated with underlying diseases like SLE [2], hypertension [3,4], Moya Moya [5], AVM [6]. This entity is challenging both diagnostically and therapeutically. The diagnosis is often missed on CT angiography and their treatment through surgical access is challenging [7] and may be associated with complications. In the present covid era, there has been an increase in the association of cerebrovascular accidents with covid infection [8-10]. It has a predilection for younger patients with concurrent systemic inflammation and can present either as embolic, thrombotic infarcts, or venous thromboembolism. Both ICH bleeds in a covid patient and Charcot aneurysm is not quite well understood. We would like to discuss on whether covid status act as an aggravating factor or simply a chance association.
Case history
A 45-year-old male patient known case of hypertension on irregular medication presented with a history of sudden onset of loss of consciousness associated with multiple episodes of vomiting following which he was taken to a nearby hospital. An NCCT brain revealed right basal ganglia bleed. Subsequently, the case was referred to our center on the same day. There was no history of fever, cough, shortness of breath, or head trauma. On evaluation, the patient was found RT- PCR positive for SARs-CoV-2 and was subsequently shifted to covid ICU. Patient GCS was poor (E2V2M4) with sustained high blood pressure. The patient’s vitals are as follows – temperature 100.60F, pulse 127 bpm, SpO2 was 92 % at room air and oxygen support @ 2-4 L/min was given. Patients RBS (331 mg/dl) and bilirubin (3 mg/dl) were raised. The CT brain angiography showed a positive “Spot sign” in the right basal ganglia (Figure 1 A-F). Before the subsequent intervention, the patient succumbed on the third day after admission.
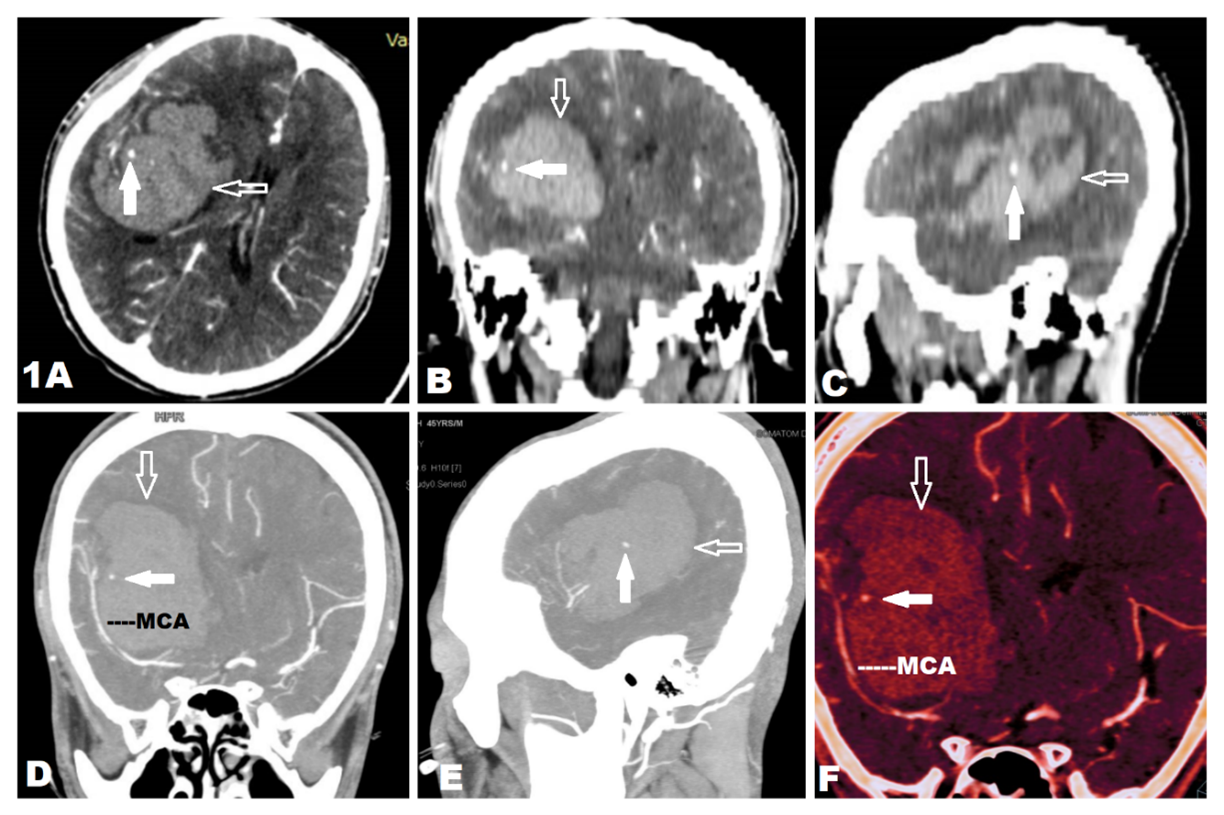
Figure 1. CECT of a 45-year-old male with intracranial bleed (open arrow) due to rupture of Charcot Bouchard’s aneurysm (solid arrow)- “Spot sign”. A, B and C. Axial, coronal and sagittal CT scans showing the intraparenchymal bleed (open arrow) in the right frontotemporal lobe. D and E. MIP images in coronal and sagittal reconstruction showing the ruptured aneurysm supplied by the right middle cerebral artery (MCA). F. VRT images in coronal reconstruction showing the ruptured aneurysm in the right MCA territory
Discussion
Rupture of lenticulostriate aneurysms is one of the rare causes of intracerebral hemorrhages. Very less literature works is noted describing the possible natural course of these lesions. An early study by Coles and Yates [3] stated that microaneurysms formed as a result of the aging process and were accelerated with hypertension. However, since then the entity has been controversial. Some investigators found no true aneurysms in the ICH patients. On pathological evaluation pseudoaneurysms, lipohyalinosis, and dissecting aneurysms were found [3,11,12].
In a new study on Charcot Bouchard aneurysm in 2021 [13], the pathogenesis of these aneurysms was described. Due to the shear force, chronic hypertension resulted in smooth muscle hypertrophy which led to fibrinoid necrosis and sclerosis of the media. They were replaced by hyaline and these hyalinized low-pressure areas were prone to develop aneurysms and ultimately rupture. The lenticulostriate arteries are predominantly susceptible to rupture due to poor pressure capacity [14]. Following bleeding into the deep structures apart from the mass effect several inflammatory pathways are activated. One of the pathways is by activating the clotting cascade leading to increased thrombin and increasing the pro-inflammatory states.
In our case, a diagnosis of rupture of distal lenticulostriate artery was made based on the “Spot sign” on CT angiography. One of the potential etiology leading to this appearance is the Charcot Bouchard microaneurysm [15]. The enhancing focus may be attributed to the pooling of contrast around the ruptured aneurysm similar to the process of contrast extravasation.
The COVID microangiopathy and coagulopathy presenting as cytokine storm leading to endothelitis and vasculitis are recognized as a mechanism of ICH [16]. In a new study on covid related intracranial bleed in 2020 [17], few conclusions were derived related to the natural course. They found that the hemorrhage occurred in younger patients less than 50 years which in all cases were lobar in location except one. Mean 30 days was reported between covid symptoms and ICH bleed. Hence though hypertension and diabetes mellitus are independent risk factors for the development of ICH in a covid patient [18], based on the period we cannot attribute the bleed in our case due to covid.
Conclusion
This case reiterates the importance of CT angiography to rule out the structural cause of vasculopathy as a cause of ICH in a young patient even with risk factors like hypertension and diabetes mellitus. A possible cause of covid associated bleed may also be excluded due to the time of presentation and location of the bleed.
Declaration
Funding: Nil.
Conflicts of interest/Competing interests: All authors declare no conflicts of interest.
References
- Hinojosa-Gonzalez DE, Ferrigno AS, Martinez HR, Farias JS, Caro-Osorio E, et al (2021) Aneurysms of the Lenticulostriate Artery: A Systematic Review. World Neurosurg 145:471-479. [Crossref]
- Kidoguchi J, Chiba M, Murakami T, Saiki I, Kanaya H, et al (1987) A case of systemic lupus erythematosus associated with an aneurysm of the lenticulostriate artery. No Shinkei Geka 15:1221-1225. [Crossref]
- Cole FM, Yates PO (1967) The occurrence and significance of intracerebral micro-aneurysms. J Pathol Bacteriol 93:393-411. [Crossref]
- Cole FM, Yates P (1967) Intracerebral microaneurysms and small cerebrovascular lesions. Brain 90:759-768. [Crossref]
- Murakami H, Mine T, Nakamura T, Aki T, Suzuki K (1984) Intracerebral hemorrhage due to rupture of true aneurysms of the lenticulostriate artery in moyamoya disease. Case report. Neurol Med Chir 24:794-799. [Crossref]
- Ohta H, Ito Z, Nakajima K, Fukasawa H, Uemura K (1980) A case report of ruptured lenticulostriate artery aneurysm with arteriovenous malformation (author's transl). No To Shinkei 32:839-846. [Crossref]
- Agarwalla PK, Walcott BP, Dunn IF, Thiex R, Frerichs K, et al (2014) Fusiform aneurysms of the lenticulostriate artery. J Clin Neurosci 21:373-377. [Crossref]
- Klok FA, Kruip MJHA, van der Meer NJM, Arbous MS, Gommers D, et al (2020) Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-19: An updated analysis. Thromb Res 191:148-150. [Crossref]
- Mao L, Jin H, Wang M, Hu Y, Chen S, et al (2020) Neurologic Manifestations of Hospitalized Patients with Coronavirus Disease 2019 in Wuhan, China. JAMA Neurol 77:683-690. [Crossref]
- Markus HS, Brainin M (2020) COVID-19 and stroke-A global World Stroke Organization perspective. Int J Stroke 15:361-364. [Crossref]
- Challa VR, Moody DM, Bell MA (1992) The Charcôt-Bouchard aneurysm controversy: impact of a new histologic technique. J Neuropathol Exp Neurol 51:264-271. [Crossref]
- Takebayashi S, Kaneko M (1983) Electron microscopic studies of ruptured arteries in hypertensive intracerebral hemorrhage. Stroke 14:28-36. [Crossref]
- Gupta K, Das JM (2021) Charcot Bouchard Aneurysm. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2022.
- Pleşea IE, Cameniţă A, Georgescu CC, Enache SD, Zaharia B, et al (2005) Study of cerebral vascular structures in hypertensive intracerebral haemorrhage. Rom J Morphol Embryol 46:249-256. [Crossref]
- Wada R, Aviv RI, Fox AJ, Sahlas DJ, Gladstone DJ, et al (2007) CT angiography "spot sign" predicts hematoma expansion in acute intracerebral hemorrhage. Stroke 38:1257-1262. [Crossref]
- Tsivgoulis G, Palaiodimou L, Zand R, Lioutas VA, Krogias C, et al (2020) COVID-19 and cerebrovascular diseases: a comprehensive overview. Ther Adv Neurol Disord 13:1756286420978004. [Crossref]
- Benger M, Williams O, Siddiqui J, Sztriha L (2020) Intracerebral haemorrhage and COVID-19: Clinical characteristics from a case series. Brain Behav Immun 88:940-944. [Crossref]
- Pavlov V, Beylerli O, Gareev I, Solis LFT, Herrera AS, et al (2020) COVID-19-Related Intracerebral Hemorrhage. Front Aging Neurosci 12:600172. [Crossref]