Abstract
An in depth understanding of root canal anatomy and its variations is an important parameter for determining the clinical success of an endodontic treatment. ‘C’-shaped canal system is a peculiar anatomic variation depicting an ethnic predilection with high incidence in Asian population. This characteristic feature of root canal anatomy has been reported to occur in various teeth but most frequently observed in mandibular second molars. These canal systems are named for the cross-sectional morphology of root and root canal. Characteristic feature like presence of a fin or web connecting the individual mesial and distal canals makes the canal cross sectional and 3D shape variable along the root. Their diagnosis with routine radiographic techniques and management with respect to debridement and obturation frequently pose a challenge in front of dental clinicians. This paper presents successful endodontic management of three mandibular molar teeth with C-shaped canal system in two cases.
Key words
C-shaped root canal, mandibular second molar, fused roots
Introduction
Anatomical variations in root canal systems of different teeth frequently pose difficulties pertaining to their diagnosis and treatment even to the most experienced clinicians. ‘C’-shaped canal system is a complex anatomic variation documented by Cooke and Cox in 1979 in endodontic literature [1]. The term was proposed based on the cross-sectional morphology of root and root canal. It has been reported to show ethnic variations being more common in Asian population [2]. The prominent feature of this canal configuration is the presence of a fin or web connecting the individual mesial and distal canals which makes the canal cross sectional and 3D shape variable along the root, presenting a challenge to debridement and obturation [3]. Thus, it is imperative for every dental clinician to be familiar with this variable root canal anatomy so as to achieve a better success rate.
Present case report involves endodontic management of two cases with three mandibular molar teeth with C-shaped canal system who reported at Department of Conservative Dentistry and Endodontics of our dental centre and were treated successfully after taking necessary ethical clearance and informed consent from these patients.
Case report
Case 1
A 26 year old Indian female patient reported at Department of Conservative Dentistry and Endodontics with chief complaints of multiple decayed teeth, severe attrition, prolonged sensitivity to hot and cold with pain in the lower posterior teeth region (Left & Right). Relevant medical history including respiratory illness, systemic disease, endocrinal disorders, allergies etc of the patient was not significant. Intraoral examination presented severe attrition of teeth, multiple carious teeth, pulp exposures with respect to 37 and 47 regions. Both these teeth were abnormally responsive to hot and cold vitality tests. Ortho pantomogram view (OPG) of the patient showed generalized reduced remaining thickness of dentin, multiple radiolucent areas with respect to various teeth. Radiolucent areas encroaching upon pulp space were observed with respect to 37 and 47 region depicting pulp exposures. Both these contralateral mandibular second molar teeth presented with some additional radiographic features such as single conical fused roots, large and deep pulp chamber, mesial and distal root canals joining at apical third level (Figure 1a & 1i).
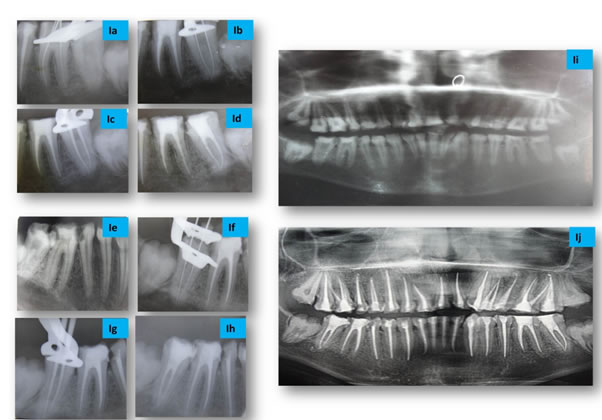
Figure 1. Radiographic IOPA View of Case- 1 (37 & 47 Region) : (Ia & Ie) Diagnostic view showing single conical fused roots, large and deep pulp chamber, mesial and distal root canals joining at apical third level, (Ib & If) Working length with converging files at apical third level (Ic & Ig) Master cone, (Id & If) Post obstruction, (Ii & Ij) Pre and post operative OPG view
These findings suggested the presence of C‑shaped canal anatomy in both the teeth. The patient was diagnosed with irreversible pulpitis with respect to 37 and 47region. Full mouth rehabilitation was planned using PFM crown restorations after root canal treatment of all the teeth.
After taking an informed consent, under profound anaesthesia and proper isolation with rubber dam, an access cavity was prepared in 37. Pulp chamber was irrigated using copious amount of 5% NaOCl also as to debride and identify the pulp chamber floor clearly. An unusual anatomy with a large and deeply situated C-shaped pulp floor with two orifices (one mesial and one distal) was observed after careful probing. Working length was determined with K-files using apex locater (Root ZX, J. Morita, USA) and IOPA radiographs. Radiographic examination revealed files joining at the apical level (Figure 1b). Cleaning and shaping were done with Coltene Hyflex CMrotary files (Coltene Whaledent, USA) up to size 30 (0.06 taper) using crown down technique followed by use of small K-files in isthmus areas assisted with ultrasonic passive irrigation (5% NaOCl). Ca (OH)2 (RC-Cal, India) was placed as an intracanal medicament.
During next appointment (after one week) master cone IOPA radiograph was taken with master Cone Gutta-Percha (Figure 1c) and obturation done with master cone along with accessory cones and AH- plus endodontic sealer (Dentsply Maillefer Company, USA) (Fig.-Id). Same treatment procedure was followed for treatment of contralateral tooth (47 region) (Figure 1e-h). Patient was found to be asymptomatic on follow up visits after every month for six months (Figure 1i and 1j).
Case-2
A 32 year old Indian male patient reported at our Department of Conservative Dentistry and Endodontics with a chief complaint of pain and prolonged sensitivity to hot and cold in lower left posterior tooth for last few days. Relevant medical history including respiratory illness, systemic disease, endocrinal disorders, allergies etc of the patient was not significant. Intra oral examination presented deep distoproximal caries with respect to 37 regions. Tooth was abnormally responsive to hot and cold vitality tests.
Radiographic examination (Intraoral Periapical View) revealed distoproximal radiolucent area encroaching upon pulp space, specific features such as deeply situated pulp floor, closely located mesial and distal roots separated by thin radiolucent line, mesial and distal root canals joining at apical third level (Figure 2a).The race and radiographic findings of the patient suggested the presence of C‑shaped canal anatomy of this tooth. The patient was diagnosed with 37 irreversible pulpitis and planned for root canal treatment in a similar manner as mentioned in case-1.
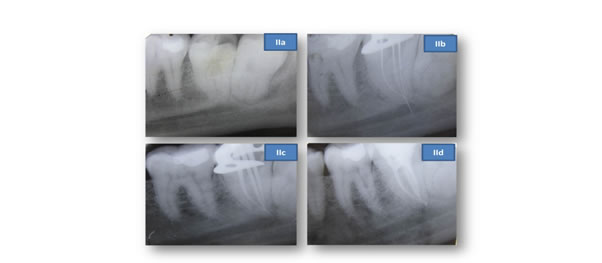
Figure 2. Radiographic IOPA View of Case- 2 (37 Region) : (IIa ) Diagnostic view showing distoproximal caries, closely located mesial and distal roots separted by thin radiolucent line, mesial and distal root canals joining at apical third level (IIb) Working length with converging files at apical third level (IIc) Master cone (IId) Post obturation
After taking an informed consent, access preparation and debridement, visual examination revealed a deeply situated C-shaped pulp floor with two orifices (one large semicolon and one round shape). On careful exploration, three canals (two mesial and one distal) were observed below these orifices. Working length Intraoral Periapical radiograph view revealed three K-files joining at the apical level (Figure 2b). Cleaning and shaping followed by obturation (Figure 2c & 2d) was done as mentioned in case-1. Patient was found to be asymptomatic on follow up visits of six months for one year.
Discussion
C-shaped canal system is a complex anatomical variation reported in various human teeth such as mandibular first premolar [4], mandibular first molar [5], maxillary first molar [6] and maxillary second molar [7], but occurs most frequently in mandibular second molars [8]. This configuration shows an ethnic predilection with high incidence in Asian population [2]. East Asian population groups like China (0.6%-41.27%) and Korea (31.3%-45.5%) have shown a high prevalence of this anatomic variation. It has also been reported to be prevalent at much higher rate in Burmese population (22.4%) than the Indian, Thai or Sri Lankan population amongst South Asian countries. Similarly, a higher incidence of C-shaped anatomy was documented in Lebanese population (19.1%) as compared to the other West Asian population groups (Iranian, Jordanian, Saudi Arabian) [9].
Present case series involves all the teeth depicting C-shaped canal configuration in mandibular second molars. Case-1 showed bilateral occurrence of C-shaped canal anatomy in mandibular second molar which has been reported in 70% - 81% of the cases [9]. Intra oral radiography in the form of radiovisiography (a type of direct digital radiography) offers many advantages over conventional radiography. However, it has the limitation of identification of image features buried in a background of normal anatomic structures (noises) [10]. CBCT is another imaging technique widely used in endodontics. But this technique should be used only when adequate diagnosis using conventional dental radiography or alternate imaging modalities is not possible [11].
Conventional intraoral radiographic techniques using silver halide film is a commonly used method for determining the canal anatomy [12]. This procedure is more beneficial in evaluating root canal anatomy and its variations like C-shaped canal system when films are used with combination technique (Preoperative, Working length and Final radiographs) [3]. Hence the similar technique was used for diagnosis in present cases. Radiographically, such teeth may present as single fused root or as two distinct roots with a communication. The latter may not be clearly visible on the radiograph giving appearance of two distinct roots. A large and deep pulp chamber is also usually observed in these teeth [9]. Diagnostic IOPA radiograph of contralateral mandibular second molars in case -1 revealed single conical root whereas radicular proximity of two roots with three radiolucent canals outline joining at apical third of the root was observed in case-2 along with a large and deeply situated pulp floor. Canal negotiation in teeth with C-shaped canal anatomy may present characteristic features on the radiographs such as instruments converging at the apex and/or exit at the furcation resembling perforation of furcation [3]. Working length IOPA radiographs showed the former feature of converging the K-files in Case -1 teeth and latter in case-2.
Diagnosis of such teeth can be made based on specific clinical findings like peculiar anatomy of pulp floor, persistent hemorrhage or pain when separate canal orifices are observed and narrow root grooves causing localized periodontal disease [3]. C-shaped orifice anatomy might reflect significant variations in different teeth. Melton et al proposed three categories of C- shaped canal system based on the cross-section shape namely continuous C shape (Category-I), semicolon shape (Category-II) and two or three discrete orifices (Category-III). Also, they reported that second type of anatomy is the most common [3]. Close observation of the pulp floor presented with two discrete orifices in Case-1whereas case -2 showed thin dentin connection separating the large semicolon shaped orifice with a small round orifice. Based on the clinical picture of pulp floor anatomy, case-1 and case-2 were classified in Category-III and II respectively.
Management of C- shaped canal system includes identification of canal anatomy using deep orifice preparation and careful probing with small files. Use of sophisticated equipments such as surgical operating microscope is also recommended for this purpose as it can facilitate the localization and handling of additional canals due to lighter and considerably higher magnification of the field of view [13-15]. It is suggested that the orifice portions of the slit be significantly widened but not deeply towards the apex so as to avoid perforation [3].
Mandibular molars with C-shaped root canals have been reported to be associated with higher percentage of uninstrumented canal areas (59.6%) using NiTi rotary instruments than manual K-file group (41.6%) [16]. NiTi rotary instrument seem to be safe in such canals and recommended to an apical dimension not greater than size 30(0.06taper). It could be followed by use of K-files or H-files specifically directed towards the isthmus areas assisted by ultrasonic irrigation to obtain better debridement [9]. Use of thermo plastic izedgutta percha technique is considered to be better for obturation in canal irregularities3. However lateral condensation technique was employed in present cases because of its wide usage in clinical practice. We found excellent results with gutta-percha and AH Plus sealer in such complex root canal variations.
Conclusion
C-shaped canal system is a complex anatomical variation showing ethnical predilection with high prevalence rate in mandibular second molars. Prognosis of such difficult cases can be improved by acquiring better understanding amongst clinicians pertaining to characteristic features, diagnosis and effective management techniques.
References
- Cooke HG, III, Cox FL (1979) C-shaped canal configurations in mandibular molars. J Am Dent Assoc 99: 836-839. [Crossref]
- Yang ZP, Yang SF, Lin YC, Shay JC, Chi CY (1988) C-shaped root canals in mandibular second molars in a Chinese population. Endod Dent Traumatol 4: 160-163. [Crossref]
- Jafarzadeh H, You-Nong Wu (2007) The C-shaped Root Canal Configuration: A Review. J Endod 33: 517-523. [Crossref]
- Baisden MK, Kulild JC, Weller RN (1992) Root canal configuration of the mandibular first premolar. J Endod 18: 505-508. [Crossref]
- Bolger WL, Schindler W (1988) A mandibular first molar with a C-shaped root configuration. J Endod 14: 515-519.
- Newton CW, McDonald S (1984) A C-shaped canal configuration in a maxillary first molar. J Endod 10: 397-399. [Crossref]
- Carlsen O, Alexandersen V (1997) Root canals in two-rooted maxillary second molars. Acta Odontol Scand 55: 330-338. [Crossref]
- Jin GC, Lee SJ, Roh BD (2006) Anatomical Study of C-Shaped Canals in Mandibular Second Molars by Analysis of Computed Tomography. J Endod 32: 10-13. [Crossref]
- Fernandes M, De Ataide I, Wagle R (2014) C-shaped root canal configuration: A review of literature. J Conserv Dent 17: 312-319. [Crossref]
- Fan W, Fan B, Gutmann JL, Fan M (2008) Identification of a C-shaped Canal System in Mandibular Second Molars—Part III: Anatomic Features Revealed by Digital Subtraction Radiography. J Endod 34: 1187-1190. [Crossref]
- Kato A, Ziegler A, Higuchi N, Nakata K, Nakamura H, et al. (2014) Aetiology, incidence and morphology of the C-shaped root canal system and its impact on clinical endodontics. Int Endod J 47: 1012-1033. [Crossref]
- Cheung LHM, Gary SPC (2008) Evaluation of a Rotary Instrument Method for C- Shaped Canals with Micro-computed Tomography. J Endod 34: 1233-1238. [Crossref]
- Sempira HN, Hartwell GR (2000) Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: a clinical study. J Endod 26: 673-674. [Crossref]
- Gorduysus MO, Gorduysus M, Friedman S (2001) Operating microscope improves negotiation of second mesiobuccal canals in maxillary molars. J Endod 27: 683-686. [Crossref]
- Cohen S, Hargreaves KM (2007) Pathways of the pulp. 9th ed. Rio de Janeiro: Mosby Elsevier.
- Kadam NS, de Ataide N (2013) Management of C‑shaped canals: Two case reports. J Orofac Sci 5: 37-41.