There has been a global push for end open defecation (OD) or achieve open defecation free (ODF) society as a matter of hygiene and sanitation. Nigeria had embraced the ODF concept and implemented some programs. The objectives of this seminar paper are to present overview of OD including prevalence in Nigeria relative to the global statistics, and review of the milestone of ODF program in the country. Stakeholders’ evaluation and outline of the factors determining success of ODF program are also presented. Implications and possible strategies for health promotion to advance ODF agenda are highlighted.
Primary healthcare, open defecation, epidemiological factors
Open defecation (OD) is a human act of defecating openly in exposed areas such as in bushes, farms, waterways, or drains without appropriate disposal of the excreta. OD is a serious environmental health hazard affecting the third world countries such as India and the Sub-Saharan Africa [1]. In Nigeria, open defecation free (ODF) program has long been adopted, but there is still much to be done [2,3]. In the recent policy briefing report [4], only 27/774 (3.49%) local governments in Nigeria have been declared ODF and none from Bayelsa state is included.
According to the United Nations agency report [5], up to 673 million people worldwide are practicing OD and 91% of them live in rural areas, as well as in Sub-Saharan African countries including Nigeria. Most of those practicing OD, do so because of a variety of reasons including but not limited to lack of access to good toilet, and poor behavior on non-utilization of available facility [6]. Further, the United Nations Children Emergency Fund (UNICEF), articulated the impacts on children health as reason to get involved in the ODF agenda [7].
It is known that good simple hygienic practice of washing hands with soap after defecation could save up to 800,000 lives from diarrhoea every year [5]. However, it probably still needs to be advanced that OD as a matter of sanitation behaviour is integral to the reduction of disease transmission. This is especially as owning a latrine at home may not necessarily stop OD in the bush or near waters [6].
Epidemiology: Prevalence of OD in Nigeria
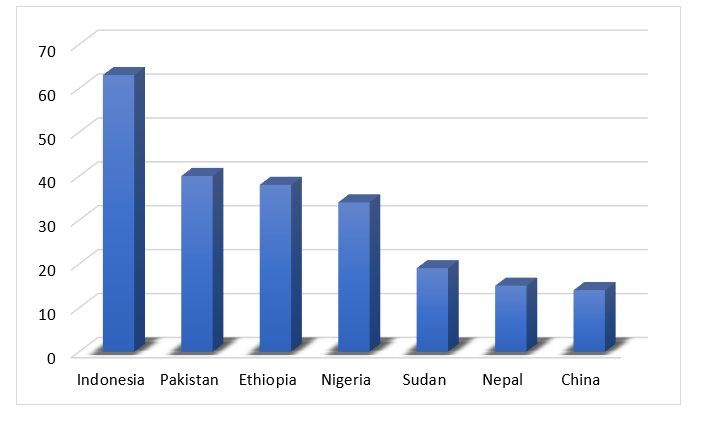
It is estimated that about 775,000 deaths per year are attributable to poor sanitation in the world [8]. Health promotion i.e., awareness campaign on the link between OD and diseases has been one of the major means of reducing the trend [9]. According to the World Health Organization and UNICEF (2012), Nigeria was ranked 5th among countries that were practicing open defecation while India topped the rank with 626 million people (Figure 1).
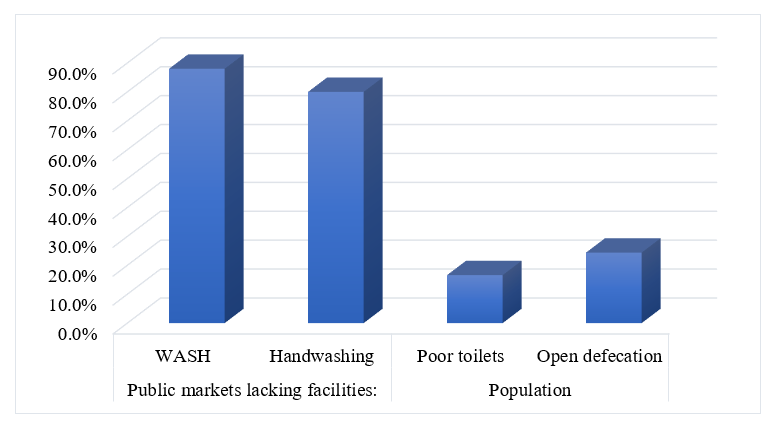
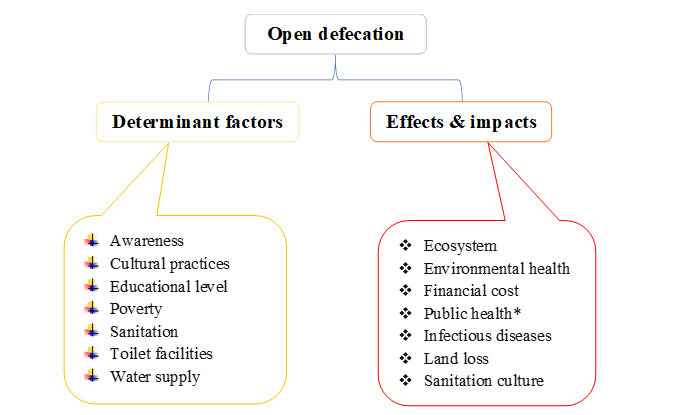
According to a more recent and scathing report [3], Nigeria seems to have become the second highest population (after India) practicing OD worldwide. The report highlights poor toilets at homes and vastly lack thereof at public markets as some epidemiological factors (Figure 2). This indication of Nigeria being second in the world differs a bit from the 2018 research report that puts the country third behind India and China [2]. It calls for a more robust review of progress made in the country’s ODF program.
With reference to the Niger Delta region (i.e., coastal communities) where Bayelsa State belongs, it has been noted that people traditionally defecate into surface waters as well as in bushes. This traditional behaviour is attributed to lack of access to sanitation facilities [2]. Indeed, a purposive field survey show that OD at these places is still being practiced, especially by travellers who stop indiscriminately when pressed and those attending markets where there is no toilet [3]. Therefore, given the advanced level of public health knowledge, it is important to review the ODF milestone.
Evaluation of stakeholders on ODF – 18 years milestone highlight
There are a lot of stakeholders who play major roles and others working in partnership or supportive role ensuing an end to OD. These amongst others include the World Health Organization (WHO), UNICEF, Ministries of Health, Agriculture, Environment, Lands, Education, Communities, and Water Resources; as well as non-governmental organizations (NGOs). Their roles differ significantly; some provides finance, sanitation marketing, education for behavior change, provision of expertise advice and other public services [10].
By far the great majority of people practicing OD live in rural areas, but this number is declining. It is probably confounding but worth noting that because of the rapid increase in the urban population, OD is still being practiced. It is worth noting that because of the rapid increase in the urban population, OD is still being practiced. Empirically, it has been noted what while rates of OD are falling globally, the same cannot be said in absolute numbers that are contrarywise increasing. For instance, it has been reported that while the proportion of global population doing OD declined from 25% in 1990 to 17% in 2008, there was increase in absolute numbers from 188 to 224 million in the same period [11]. A decline in open defecation rates was recorded in all regions.
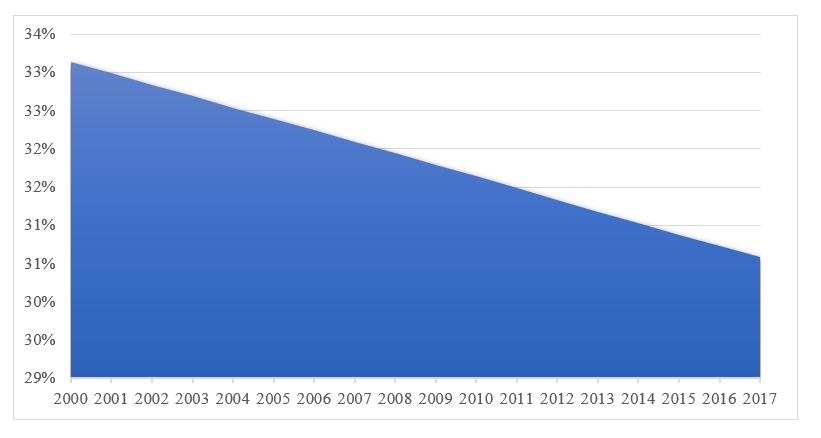
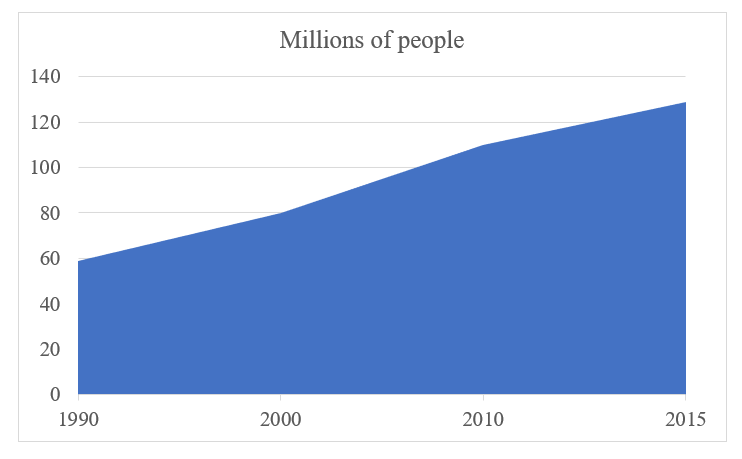
In a review of landmark achievement on OD based on data from WHO [12], Nigeria has recorded a slow and steady decline in percentage population practicing open defecation over the 18 years’ period of 2000 to 2017 (Figure 3a). However, another report has indicated consistently increasing millions of Nigerian people without appropriate sanitations since 1990 (Figure 3b). The significance of this contrasting positive and negative trends is that focus on OD decline alone could be misleading i.e., counter-productive in achieving the ODF target.
Stakeholders attempt on ODF Nigeria
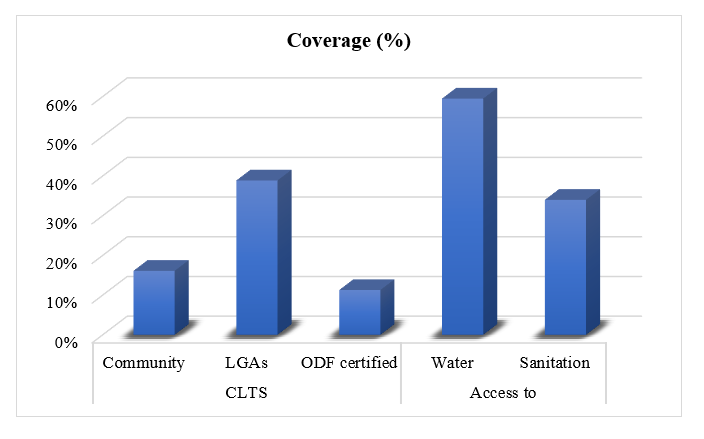
The Nigerian water sanitation and hygiene (WASH) watchdogs have been decrying the practice of OD. According to reports, only 27 local government areas have been declared as having achieved or attained ODF status, which represents less than 3.5% of the 774 LGAs in the country (Figure 4). Nigeria had a commitment to meet the MDGs of 65% sanitation coverage (improved sanitation) by 2015. Therefore, this target is yet to be achieved (Figure 4). Instead, the preceding Figure 3 highlights increasing millions of people without improved sanitation facilities. Thus, even the United Nations vow [13], or the national road map [14], i.e., of ODF Nigeria may be a far cry to attain.
Out of the approximately 123,240 communities in Nigeria, out of the 123,240 communities found in Nigeria, CLTS has been carried out in 19467 communities only which works out to less than 16%. Source? Covering the remaining communities will be a big task. Of the communities implementing CLTS, some seem to have the associated WASH program yet to be initiated and only a few have been declared ODF (Figure 4). This only shows the challenge that lies ahead and the need to assess community stakeholders [14].
A region-wide analysis of the progress on CLTS implementation, further brings out the status of CLTS in the six geo-political regions of the country. As may be seen from the percentage of communities declaring ODF is highest in South-East (78%) followed by North-Central (65%) and North-East (57%). The remaining three regions show less progress, in terms of communities declaring themselves as ODF. However, when it comes to the percentage of communities ultimately certified for ODF, the situation is different. Though, the North-East Region, where only 30% of communities reported ODF has the highest rate of certification (57%) whereas, South- East, where 78% of communities reported ODF has the lowest certification rate of 10% (Table 1) [15].
Table 1: CLTS coverage and success rates in the regions [14].
Ministry of Water Resources Abuja (2014)
Factors and impacts of OD and implication for health promotion
There is still prevalence of poor environmental health issues, especially lack of good water supply and poor sanitation, which are associated with open defecation; hence “ensuring the uniform healthcare practices” remains a primary healthcare promotion agenda [16]. Nations have adopted the campaign of “toilets before temples” [13]. As the Nigerian population continues to increase, health promotion efforts “to ensure that open defecation does not increase” is acknowledged as imperative; and this effort goes beyond ministry of health to include other stakeholders such as environmental officers and water supply services [5].
With regards to health promotion, the burden of disease cannot be over-emphasized. For this mini-series, it suffices to focus on maternal and child health. The involvement of UNICEF is an indication on impact on children [7,10]. Also, the systematic review by Saleem et al. indicates interests on maternal health impacted by OD [1].
OD seems a pandemic causing medical issues that constitutes part of contemporary public health challenges affecting socio-economic development in the affected nations. OD and its attendant medical problems are rampant in most rural communities with more efforts or programs required to overcome it. OD is in practice, because many women especially mothers do not know how to dispose of their children’s faeces safely and most people defecating in roadsides, bushes, near water sources and agricultural fields. Therefore, OD as a social health threat is very hard to eliminate from the larger culturally bound society. Thus, the target of achieving sustainable development goal of ‘clean water and sanitation’ is mere dream and becoming very hard. The effort taken need to fetch fundamental changes in the minds – i.e., address the behavioural change wheel – of the people to bring healthy transformation in our society.
This was a piece of seminar presentations on contemporary public health issues done as part of academic exercise by CNO. First review was by HEC and EUN. Second review and articulation were done by OCC and EUN.
- Saleem M, Burdett T, Heaslip V (2019) Health and social impacts of open defecation on women: a systematic review. BMC Public Health 19: 158. [Crossref]
- Abubakar IR (2018) Exploring the determinants of open defecation in Nigeria using demographic and health survey data. Sci Total Environ 637-638: 1455-1465.
- Adedigba A (2021) Nigeria worst African country in open defecation, second globally – Report.
- Okuku MO (2020) Policy brief: Ending open defecation in Nigeria. Int J Trop Dis Health 41: 47-54.
- Water Supply and Sanitation Collaborative Council and Florio J (2020) Transformational benefits’ of ending outdoor defecation: Why toilets matter.
- World Health Organization (2005) Fact sheets on environmental sanitation - Fact sheet 3.2: Open-air defecation.
- UNICEF (2021) UNICEF’s game plan to end open defecation.
- Ritchie H, Roser M (2019) Sanitation.
- Patil SR, Arnold BF, Salvatore AL, Briceno B, Ganguly S, et al. (2014) The effect of India's total sanitation campaign on defecation behaviors and child health in rural Madhya Pradesh: a cluster randomized controlled trial. PLoS Med 11: e1001709. [Crossref]
- World Health Organization (2021) Water sanitation hygiene - Fast facts: WHO/UNICEF joint monitoring report.
- Anuradha R, Dutta R, Raja JD, Lawrence D, Timsi J, et al. (2017) Role of community in Swachh Bharat Mission. Their knowledge, attitude and practices of sanitary latrine usage in rural areas, Tamil Nadu. Indian J Community Med 42: 107-110. [Crossref]
- World Health Organization (2020) Population practising open defecation.
- Deen T (2014) UN vows to eliminate open defecation by 2025.
- Federal Government of Nigeria and UNICEF (2021) Making Nigeria open defecation free by 2025: A national road map.
- Institute of Development Studies. Nigeria, 2021.
- Rahman M, Chowdhury S (2018) Primary care: The challenges of a changing world.