A 27-year-old male presented to the Emergency Department (ED), with three months history of progressive pain, bulging, and redness in his right eye (Figure 1-3). There was no history of trauma to the right eye and no previous known co-morbidities.
Figure 1. Orbital lymphangioma
Figure 2. Orbital lymphangioma
Figure 3. Lymphangioma MRI 3
Patient was alert and hemodynamically stable with right eye exophthalmos, erythema, restricted ocular movements, ectropion of the lower lid and protrusion of conjunctival sac. Visual acuity was intact in both eyes. The remaining neurological, cranial nerves and systemic examination was unremarkable.
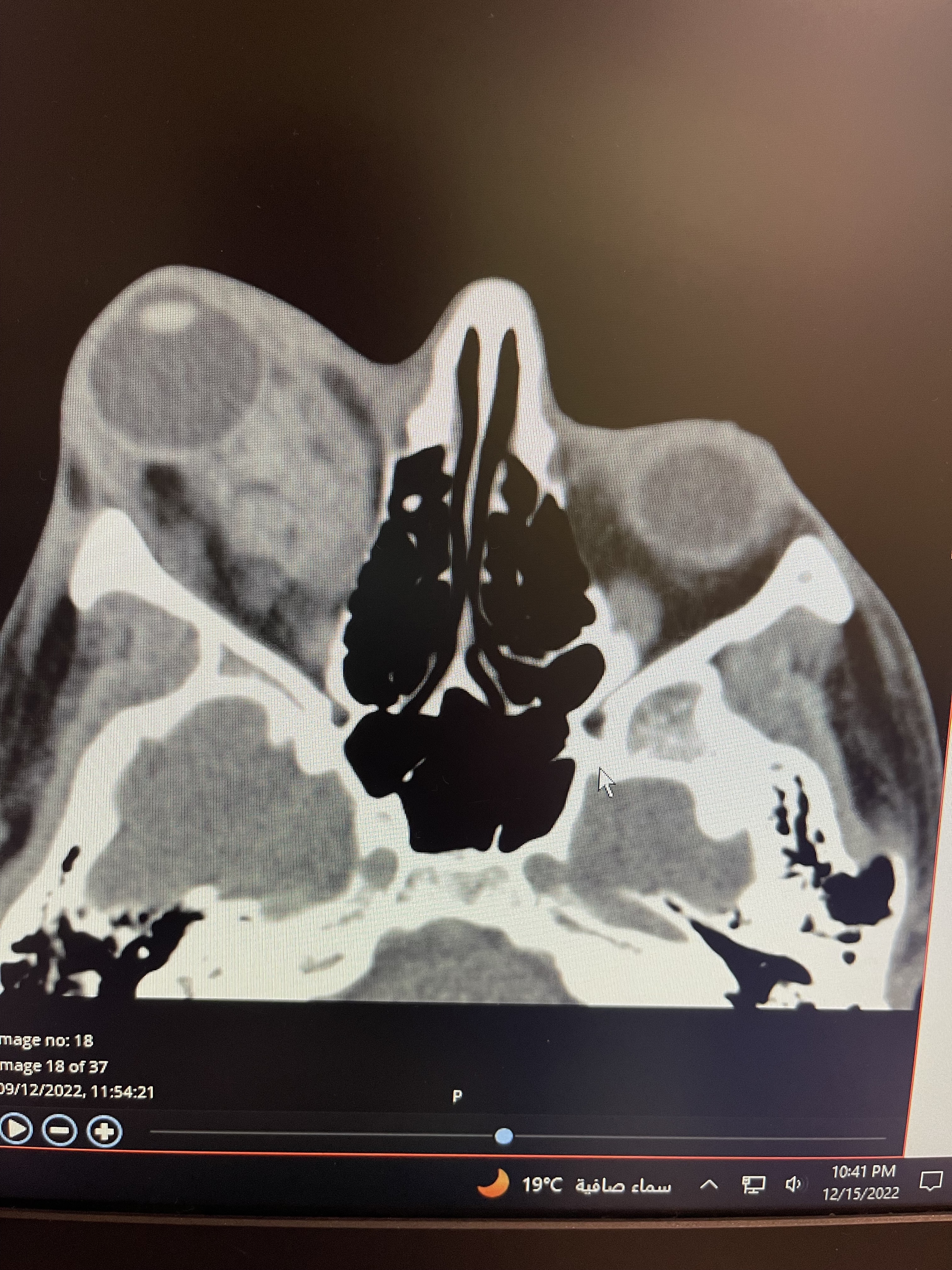
Computed Tomography (CT) scans of the right orbit showed a homogenous soft tissue mass occupying the right intra-conal compartment, with extra-conal extension on the medial aspect and inflammatory changes in the pre-septal area of right inferior eyelid. The CT brain did not show intracranial extension. Later the Magnetic Resonance Image (MRI) showed lymphatic malformation forming a soft tissue mass in the right orbit, suggestive of lymphangioma (Video 1 and 2).
Video 1. Lymphangioma MRI 1
Video 2. Lymphangioma MRI 2
Patient was discharged from the ED on analgesics and antibiotics with a follow-up appointment with ophthalmology. Patient underwent ultrasound-guided sclerotherapy, with bleomycin. Two months following the sclerotherapy, patient was recommended to start medical therapy with sirolimus, due failure of sclerotherapy. Surgical resection eventually had to be carried out after failure of medical management.
Introduction
Lymphangioma is an uncommon lymphatic malformation that can be congenital or acquired. It presents with a wide range of clinical manifestations, and mostly affects the paediatric age group. Lymphangiomas are dilated lymphatic vessels, and are visualised as multiloculated cystic lesions [1]. In recent years, there has been rapid advances in our understanding of the molecular pathology of lymphangiomas. The occurrence of lymphangiomas is associated with several signalling pathways and inhibitors that target these pathways, which are being tested in clinical trials to treat the disease. Currently, lymphangiomas are broadly classified based on clinical manifestations and complications. However, this classification is not sufficient for selecting therapeutic strategies or predicting prognosis. The management of orbital lymphangiomas can vary from simple observation to surgical intervention. Overall, there are four main treatment options; observation, sclerotherapy, medical, and surgical intervention [2].
Depending on the clinical classification and location of the lymphangioma, its clinical management and outcome can range from spontaneous regression to severe sequelae, despite comprehensive treatment [3].
Discussion
Lymphangiomas are benign malformations of the lymphatic system. Lymphangiomas can be broadly classified as either congenital or acquired lymphatic system abnormalities. In the congenital form, lymphatic channels are improperly connected to the main lymphatic drainage duct, before the age of 5 years [4]. Acquired lymphangiomas usually occur when previously normal lymphatic drainage is interrupted by surgery, trauma, malignancy, or radiation therapy [4]. There are a wide range of clinical presentations and treatment strategies of lymphangiomas. This diversity is in part due to the molecular biological mechanisms, leading to the formation of the tumor.
Four major molecular pathways might be affected in the pathogenesis of lymphangiomas. Firstly, “PI3K/AKT/MTOR Signalling Pathway” is an essential cell proliferation and differentiation regulator. A somatic mutation in PIK3CA is the most common mutation responsible for the pathogenesis of lymphangioma, involving this signalling pathway. However, the exact mechanism remains unclear. Secondly, “VEGF-C and its receptor”, are fundamental elements of lymphangiogenesis. The literature attributes the pathogenesis of lymphangioma to an abnormal VEGF-C expression in lymphatic endothelial cells. Thirdly, mutations in “Wnt/β-Catenin Signalling Pathway” is considered to be another element of lymphangiogenesis. Lastly, “RAS/RAF/MEK/ERK signaling pathway” mutations are also considered to be responsible.
Orbital lymphangioma is most commonly diagnosed in the paediatric age group. A total of 60% are diagnosed by the age of 16 years and 43% are diagnosed before the age of 6 years [1].
Most commonly, lymphangiomas present with proptosis and ptosis of the affected eye. Other possible presentations are restricted ocular movements and mechanical blepharoptosis [5]. A study conducted on five adult patients with orbital lymphangioma noted that all of them presented with ptosis [6].
It can also present with compressive symptoms such as compressive optic neuropathy.
A case reported by Thavara, et al. reported a 68-year-old male with orbital intra-conal lymphangioma. The patient presented with decreased visual acuity and diplopia along with proptosis and restricted eye ball movement. The symptoms were triggered by trauma to the left eye, six months prior to presentation. In our case, the patient had intact visual acuity and no history of trauma to the right eye [7,8].
Another reported case is of a 38-year-old female, who was known to have ulcerative colitis. She presented with unilateral headaches and exophthalmos of the left eye, which coincided with a moderate flare-up of her inflammatory bowel disease [8]. This case denotes that the presentation of exophthalmos can be linked to a systemic disease.
Patients with no history of trauma usually report a gradual onset of symptoms, as presented with our case. Only 1-3% of orbital masses present to acute emergency setting, after a delayed period [9]. Lymphangiomas should be considered among the differential diagnoses of patients presenting with acute exophthalmos and should be investigated using CT and MRI imaging.
Another reported case is of a 48-year-old female with right orbital lymphangioma, presented with retrobulbar headache and worsening orbital pain for three months. In this case, the lesion progressed slowly over the span of one year and was entirely contained within extra ocular muscles [10]. Diagnosis of lymphangiomas is commonly done based on the patient’s clinical presentation. Confirmatory tests such as dermoscopy and biopsy are also helpful. In addition, imaging can be done to further characterise the lesion’s depth and extent [11].
Histopathologic features of a lymphangioma are distinct; it is made of numerous cyst-like networks that consist of either clear fluid, blood, or both. These cysts are lined by endothelial cells. Overall, it appears as an irregular non-encapsulated mass [12]. Ultrasonography, CT, and MRI can all help with diagnosis. Ultrasonography is mainly used as a diagnostic modality in children. CT aids in visualising the orbital wall and any calcifications within the lesion. MRI is considered as the gold standard diagnostic tool. It also aids in visualising and diagnosing hemorrhagic cystic lesions, which are seen as hyper-intense in the acute hemorrhagic stage [13]. Additional laboratory investigations can be done to rule out certain differential diagnosis.
In cases of bilateral proptosis, thyroid function tests such as the T3, T4 and Thyroid-Stimulating Hormone (TSH) levels must be performed. Other possible systemic causes include Wegener’s granulomatosis, which can be investigated by anti-neutrophil cytoplasmic antibody serum assay. Furthermore, in suspected sarcoidosis cases, serum angiotensin-converting enzyme and lysozyme assays can be performed [14].
Depending on the clinical presentation, there are four treatment options for lymphangiomas. Observation is a suitable option for patients with mild symptoms, preserved visual acuity, and no orbital deformity [2]. However, with the advancement in non-surgical treatment options, observation alone is no longer recommended [5].
Sclerotherapy is an efficient non-surgical treatment of orbital lymphangioma. It involves ultrasound-guided technique; fluid is aspirated for cytology, followed by intra-lesional injection of sclerosing agent for curative reason or to reduce the lesion size prior to surgical resection. The most commonly used sclerosants are piciabanil, sodium tetradecyl sulfate, sodium morrhuate, or bleomycin [3,15].
Although sclerotherapy showed promising results in treating lymphangiomas, it carries some serious risks, such as infections, bleeding, pulmonary fibrosis, and increased intra-orbital pressure [12,15].
Non-invasive medical therapy with sildenafil or sirolimus has been used to treat orbital lymphangioma [16,17]. Sildenafil is a phosphodiesterase inhibitor (PDE-5 inhibitor), which works by inhibiting phosphodiesterase enzymes and intervening with cyclic GMP. This results in increase in its levels within the smooth muscle cells, providing a vasodilation effect. A case series conducted by the university of California-Davis Medical Center, showed a favorable response to sildenafil in patients with extensive orbital and facial lymphangioma, who failed repeated sclerotherapy; the response was efficient, making enucleation unnecessary [18]. However, there are no sufficient studies about the length of treatment and long-term complications of sildenafil [16].
Sirolimus is an immunosuppressant and a novel therapy for orbital lymphangioma. It is a mammalian (mechanistic) target of rapamycin (mTOR) inhibitors. mTOR coordinates signals from the PI3K/AKT pathway, an essential pathway in cell growth and proliferation through organizing ribosomes and protein biogenesis. In vascular anomalies like lymphangiomas, inhibiting mTOR and blocking signals in the PI3K/AKT pathway will decrease lymphangiogenesis and angiogenesis. Sirolimus showed a favorable result, particularly in tumors with significant lymphatic components. For instance, the initial use of sirolimus for vascular anomalies was for a young patient with Kaposiform hemangioendothelioma (KHE), a rare vascular neoplasm with extensive abnormal lymphangiogenesis; this patient failed the standard therapy for KHE. This patient and five more high-risk patients responded very well to sirolimus to manage their vascular anomaly. A clinical trial studied the efficacy and safety of sirolimus in treating patients with complicated vascular anomalies, who failed standard treatment. The study summarised sirolimus-associated toxicity, mainly in the blood and bone marrow in 27% of the subjects, followed by metabolic toxicity in 3%. Moreover, other side effects have been reported, such as constitutional symptoms, peripheral edema, hypertriglyceridemia, and diarrhoea [15,19].
Surgical excision or debulking with subtotal resection can be considered as a last resort. However, the close vicinity of the lesion to vital structures such as the optic nerve and extra ocular muscles makes the surgical intervention challenging and total resection is almost impossible [17].
Conclusion
Acquired adult orbital lymphangiomas are extremely rare. They can present with acute and rapid onset eye pain and exophthalmos, without predisposing trauma or injury. There is high rate of failure of sclerotherapy and medical treatment. Orbital lymphangioma should be a differential diagnosis of acute unilateral exophthalmos.
References
Nassiri N, Rootman J, Rootman DB, Goldberg RA (2015) Orbital lymphaticovenous malformations: Current and future treatments. Survey of Ophthalmology 60: 383–405. [Crossref]
Patel SR, Rosenberg JB, Barmettler A (2019) Interventions for orbital lymphangioma. The Cochrane database of systematic reviews 5: CD013000. [Crossref]
Patel KC, Kalantzis G, El-Hindy N, Chang BY (2017) Sclerotherapy for Orbital Lymphangioma - Case Series and Literature Review. In vivo (Athens, Greece) 31: 263–266. [Crossref]
Liu X, Cheng C, Chen K, Wu Y, Wu Z (2021) Recent progress in Lymphangioma. Frontiers in Pediatrics 9. [Crossref]
Saha K, Leatherbarrow B (2012) Orbital lymphangiomas. Current Opinion in Ophthalmology 23: 433–438. [Crossref]
Simas N, Farias JP (2014) Orbital lymphangiomas: Surgical treatment and clinical outcomes. World Neurosurgery 81: 5-6. [Crossref]
Thavara BD, Rajagopalawarrier B, Balakrishnan S, Kidangan GS (2020) A Case of Adult Orbital Intraconal Lymphangioma. Asian journal of neurosurgery 15: 168–171. [Crossref]
Sayadi S, Ben Brahem M, Ben Abdallah K, Kharrat M, Ben Mohamed A, et al. (2023) Orbital cystic lymphangioma diagnosed during an ulcerative colitis flare-up in an adult woman: Association or coincidence?. Journal francais d'ophtalmologie S0181-5512: 00077-3.. [Crossref]
Seca M, Borges P, Reimão P, Gomes M, Meireles A (2012) Conjunctival lymphangioma: A case report and brief review of the literature. Case Reports in Ophthalmological Medicine 2012: 1–4. [Crossref]
Kothari P, Mirani N, Langer PD (2020) Orbital Lymphangioma Confined to an Extraocular Muscle. Ophthalmic plastic and reconstructive surgery 36: e61–e62. [Crossref]
Miceli A, Stewart KM (2023) Lymphangioma. In: StatPearls, Treasure Island (FL): Stat Pearls Publishing [Crossref]
Suzuki Y, Obana A, Gohto Y, Miki T, Otuka H, et al. (2000) Management of orbital lymphangioma using intralesional injection of OK-432. Br J Ophthalmol 84: 614–617. [Crossref]
Roman A, Bianchini L, Battistel B, Franzoi Neto M, Schwingel D (2017) Orbital Lymphangioma: Case report and management paradigms. Arquivos Brasileiros De Neurocirurgia: Brazilian Neurosurgery36: 136–140.
Ahmad SS, Anwar R, Khan MA, Usmani N, Jahan S (2021). Evaluation of proptosis: A Primer. Ophthalmology 15: 26.
Patel SR, Rosenberg JB, Barmettler A (2019) Interventions for orbital lymphangioma. Cochrane Database Syst Rev 5: CD013000. [Crossref]
Russin JJ, Rangel-Castilla L, Kalani MY, Spetzler RF (2015) Surgical management, outcomes, and recurrence rate of orbital lymphangiomas. J Clin Neurosci 22: 877–882. [Crossref]
Lagrèze WA, Joachimsen L, Gross N, Taschner C, Rössler J (2019). Sirolimus-induced regression of a large orbital lymphangioma. Orbit (Amsterdam, Netherlands 38: 79–80.
Gandhi NG, Lin LK, O'Hara M (2013) Sildenafil for pediatric orbital lymphangioma. JAMA Ophthalmol 131: 1228-1230.
Adams DM, Trenor CC 3rd, Hammill AM, et al. (2016) Efficacy and Safety of Sirolimus in the Treatment of Complicated Vascular Anomalies. Pediatrics 137: e20153257.
Editorial Information
Editor-in-Chief
Guo-Gang Xing
Perking University
Article Type
Case Report
Publication history
Received date: June 19, 2023
Accepted date: July 11, 2023
Published date: July 14, 2023
Qureshi MN, Hamdan DN, Hijazi RM, Aldahlan RS (2023) Orbital Lymphangioma presentation in the emergency department. Trauma Emerg Care 8: doi: 10.15761/TEC.1000227
Corresponding author
Dr Muhammad Nauman Qureshi
Dr Muhammad Nauman Qureshi, Consultant & Research director, Department of Emergency Medicine, King Faisal specialist hospital and research center, Riyadh, Saudi Arabia.