Background :Real-time three-dimensional transesophageal echocardiography or RT-3DTEE, with advances in image processing and display, has increased the availability and utility of TEE to a variety of clinical settings as diagnosis and catheter intervention.
Patients & methods :We study all Patients with RT-3DTEE, presented in MEDIC HCMC from October 2010 to May 2020.
Results :From October 2010 to May 2020, in MEDIC HCM, we have already performed 1276 cases of Real-tim 3DTEE: Mitral Stenosis ( 31% ), Atrial Septal Defects ( 16% ) and other diseases of the heart.The display of three dimensional images of 3DTEE providing important informations to assess the anatomical structures and the severity of diseases prior to perform interventional procedure.
Conclusion:Real-time 3DTEE overcomes the limitations of 2DTEE in making diagnosis and guiding the catether intervention.
Three dimensional transesophageal echocardiography, mitral stenosis, atrial septal defect
The first utilization of a TEE device that promised to have clinical utility was reported in 1976 by Frazin and coworkers, who described the application of transesophageal M-mode echocardiography.The use of this technology was subsequently reported for the evaluation of ventricular function during supine exercise.
The next success was the development of real-time, two-dimensional TEE imaging, as first described in 1980 by Hisanaga, who developed a wide-angle mechanical sector scanner, while in 1982 Schluter reported on the use of transesophageal phased-array two-dimensional echocardiography.
The incorporation of color mapping into a TEE device was first reported by investigators from Saitama Medical School in Japan. The same group was instrumental in early development of standard biplane, matrix phased -array biplane, and small pediatric probe.
The current-generation probes are all multiplane devices. Rotating the small control wheel flexes the tip to the left or to the right.But with the multiplane TEE transducer, this manipulation is rarely necessary. Rotation of the transducer refers to movement of the sector scan from 0 to 180 degrees.
Transthoracic and transesophageal real-time three dimensional echocardiography is a significant advancement in technology. Advances in image processing and display, the addition of three dimensinal imaging capability, and the portability of ultrasound system have increased the availability and utility of TEE to a variety of clinical settings as diagnosis, cardiac catetherization, operation and intensive care.
Currently percutaneous interventions for many structural diseases increase more and more in our country. Interventional cardiologists are now treating a variety of lesions that previously required surgery as mitral stenosis, aortic stenosis, ostium secundum ASD, VSD, PDA, Coronay Fistula…Although Fluoroscopy and 2D TEE are usually used for procedural guidance, real-time three-dimensional TEE offers several important advantages over these modalities.
Previously, Toshiba SSH 140 A with TEE biplan probe have been used to perform 2D TEE in our hospital. Since October 2010, transesophageal echocardiographies are made by X-MATRIX, iE 33 Philips machine.
- Role of 3DTEE in the assessment of heart diseases
- Advantages of 3DTEE in compare with 2DTEE
- Pts with 3D TEE at MEDIC HCM, Viet Nam, from October 2010 to May 2020
- 2- Instruments: X-MATRIX Philips iE33, X-7 real-time 3D TEE probe; Acquision mode including Live 3D or narrow sector, Full Volume or wide sector, Zoom or the smallest pyramydal size available for acquisition
- 3- Techniques: Explain the procedure to the patient; The patient should not have had any intake of food or drink for at least 4-6 hours. Oral prostheses should be removed. The patient should be placed in the left lateral decubitus position. Topical anesthetic and sedation, Introduce a bite block between the teeth. The probe is gently passed into the oral cavity over the tongue and guided into the larynx. The patient should be asked to swallow, the probe is gently introduced into esophagus.
- 4-Case series report study is applied for this topic.
- 5-The advantages of 3DTEE in compare with 2DTEE in diagnosis and evaluation of diseases prior to perform interventions.
From October 2010 to May 2020, in MEDIC HCMC, we have already performed 1278 cases of 3DTEE: Mitral stenosis (31%) and other valvulopathie including Mitral Regurgitation, Aortic valvulopathies, Atral Septal Defects (16%) and other shunts as PDA, VSD; then Myxoma and cardiac tumors, Endocarditis, studying prosthetic valves. The other complicated cardiopathies as Coronary artery fistula, Valsalva sinus rupture, Ebstein anomaly.
The percutaneous balloon mitral valvuloplasty, trasncatether closure of ASD and surgery have demonstrated the precised diagnosis of 3DTEE (Figure 1).
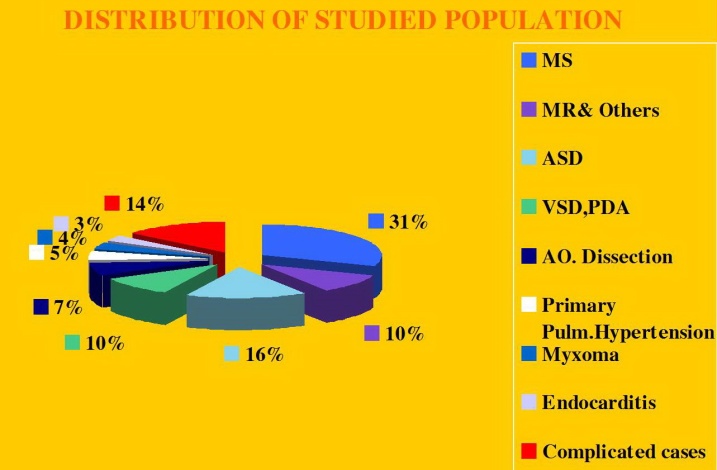
Figure 1. Distribution of heart diseases detected by RT-3DTEE
Among 396 Pts with MS, ,mean age=45 ( from 18-72 ages), the majority of patients were female (75.2%) , Dyspnea is the first symptom to the consultation, sometime embolic events (7.5%) keep patients going to their cosultants, AF account 6,1%.Rheumatic Fever is predominant cause, with important fusion of commissures (70%), 2DTEE completed by 3DTEE is used to calculate theWilkins score, providing informations more exactly than 2D TTE alone, prior to perform Balloon Mitral Commissurotomy or surgery.
MVA3D measured by Real-Time 3DTEE to compare with conventional two-dimensional planimetry MVA2D.The 3D Assessment was significantly smaller the 2D planimetry: MVA3D = 0.95cm2 ± 0.21; MVA2D =1.16cm2 ± 0.24; mean diffence=-0.21cm2, n=327, p<0,001.
Some patients with high Wilkins score evaluated by 2DTEE still have responded well to Balloon Mitral Valvuloplasty. Real-time three-dimensional transesophageal echocardiography provides important informations regarding the involvement of rheumatic process on the mitral valve, particularly the symmetry length of commissural fusion. Furthemore RT-3DTEE also shows the thickening, the fibrosis and the calcification of the whole mitral commissures that cannot be visualized by 2DTEE. The 3D image allows superior visualization of the thickening of the mitral leaflet, particularly the commissures.
The 3DTEE usually details the subvalvular apparatus not appreciated on 2DTEE while studying the leaflets.
Because patients often presented late in Hospitals, their Wilkins score usually is high (68% with Wilkins score is superior to 8). Especially, LAA thrombus, even small size, furthermore, can be detected more clearly on RT- 3DTEE. Volume and mobility of LAA thrombus appreciated better on 3DTEE.
Detection LA and LAA thrombus by RT-3DTEE is more sensitive than 2DTEE with X-plane mode and 3 D Zoom only are avaible in 3DTEE.
Direct planimetry of mitral valve orifice by 3DTEE is the gold standard method now. The cropping function ensures that the orifice area is traced in a plan that is at the tip of the mitral valve (Figures 2-17).
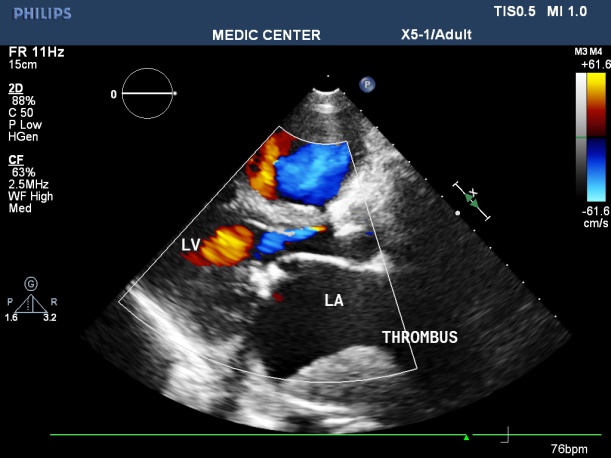
Figure 2. LAX view showing MS with severely calcified mitral leaflets& presence of LA thrombus

Figure 3. Spontaneous contrast in LAA recorded from 2DTEE
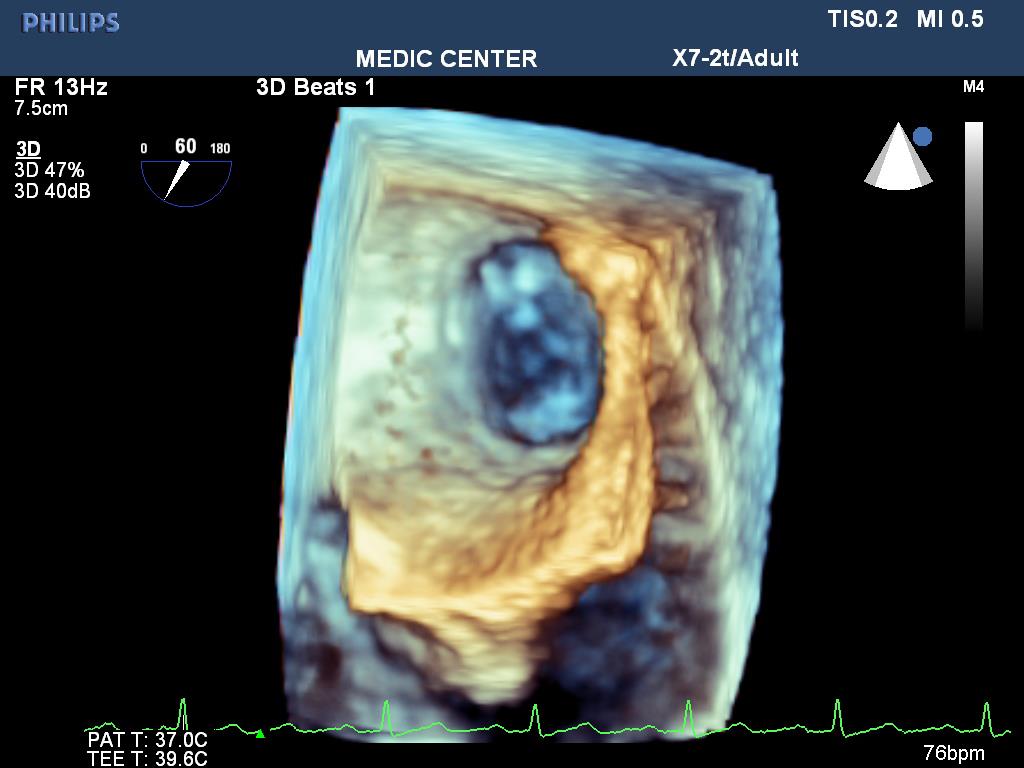
Figure 4. Normal LAA without thrombus inside, visualized by 3D Zoom
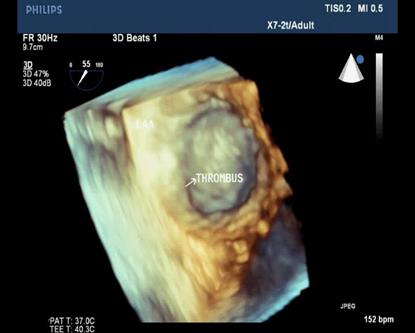
Figure 5. 3D Zoom imaging demonstrating LAA with thrombus inside
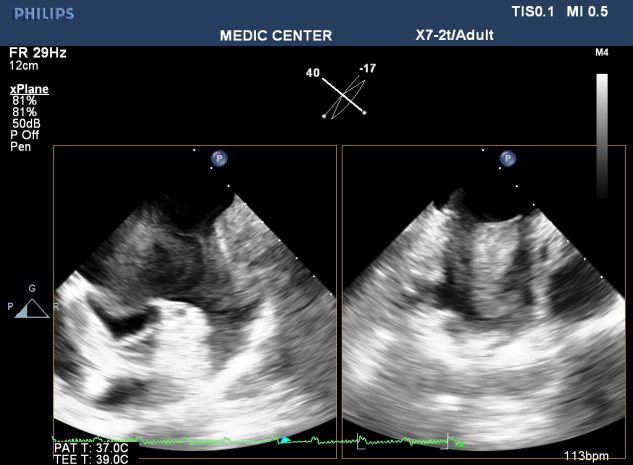
Figure 6. X-plane imaging visualizes LAA thrombus in two orthogonal planes
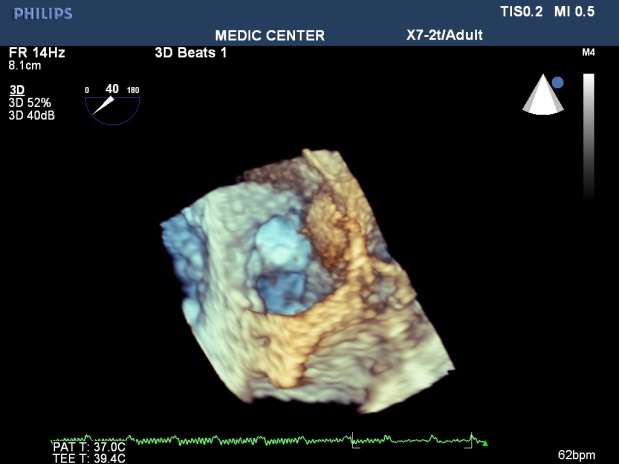
Figure 7. LAA three dimensional view with thrombus attached to LAA wall
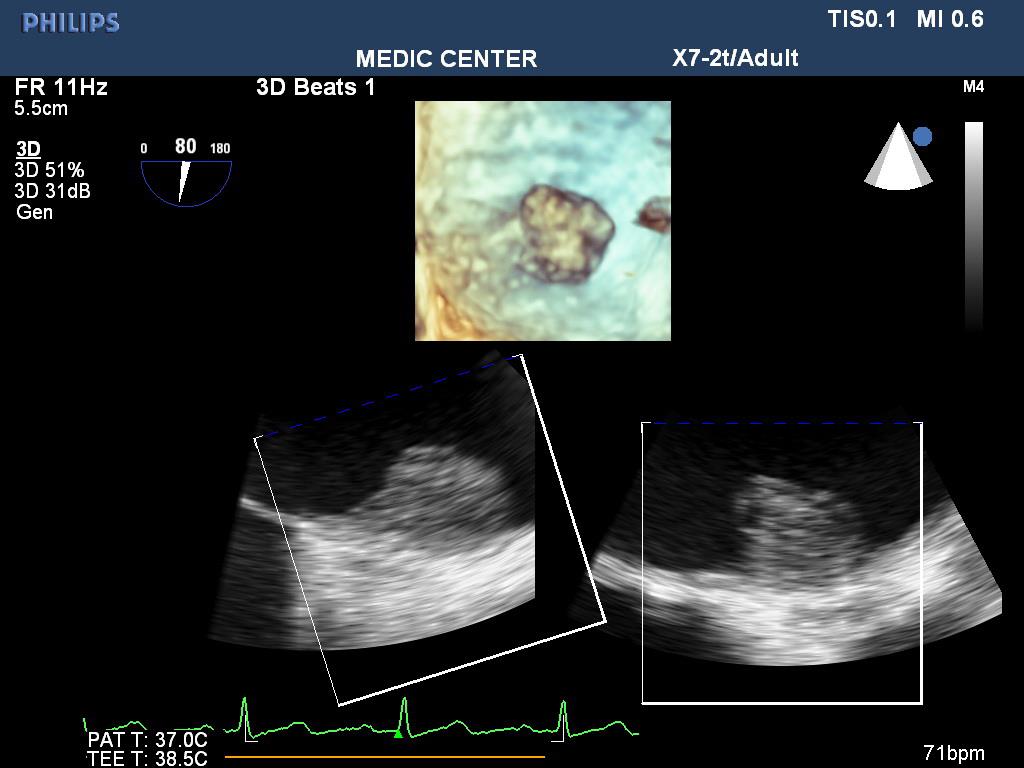
Figure 8. 3DTEE with icrop function shows thrombus attached to LA wall
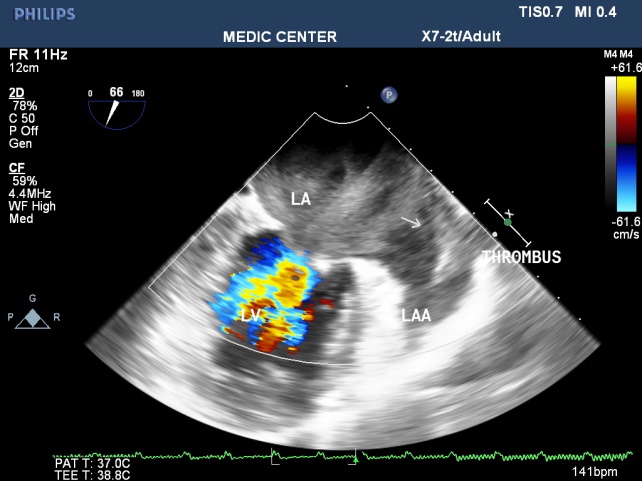
Figure 9. MS with spontaneous contrast and thrombus in LA& LAA, 2DTEE plane of 60°

Figure 10. 2DTTE parasternal LAX view shows the doming appearance of AML, thickening of subvalvular apparatus, thrombus in LA

Figure 11. 3DTTE Full volume demonstrating the restrited orifice with commissural fusion and LA thrombus

Figure 12. 2DTTE 4C view shows the 3D image of thrombus in LA

Figure 13. RT-3DTEE shows small and restrited mitral orifice, commissural fusion, extensive rheumatic nodules, severe deformity of mitral leaflets
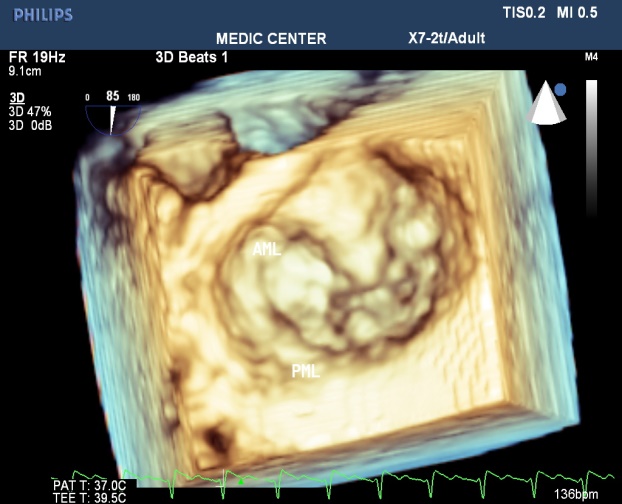
Figure 14. Zoom 3DTEE image visualizing the thickenned leaflets, commissural fusion, nodules of rheumatic fever
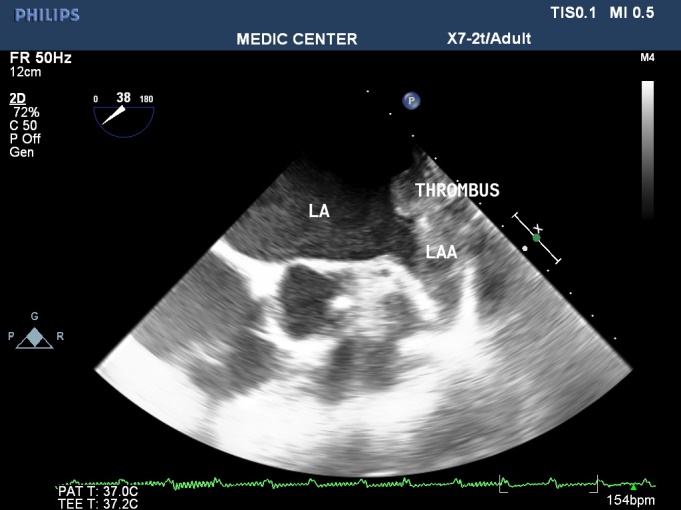
Figure 15. 2DTEE presenting LAA thrombus
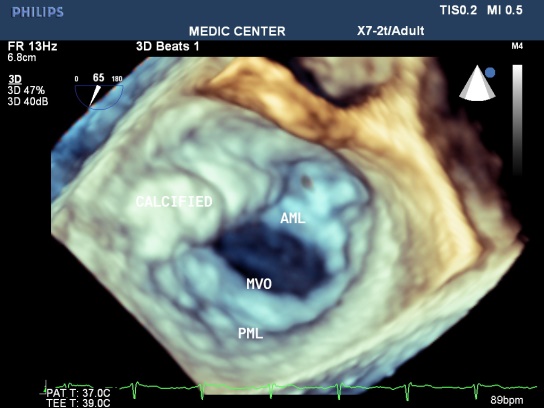
Figure 16. Zoom 3DTEE showing MS with comissural fusion and rheumatic nodules
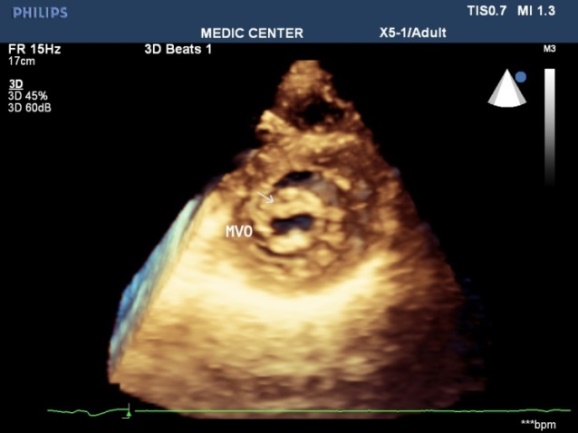
Figure 17. Parasternal 3D TTE demonstrating fusion of commissures and rheumatic nodules
Among patients with mitral regurgitation, MVP accounts for the majority of our patients, fibroelastic disease and Barlow type of MVP were seen (Figures 18-21).
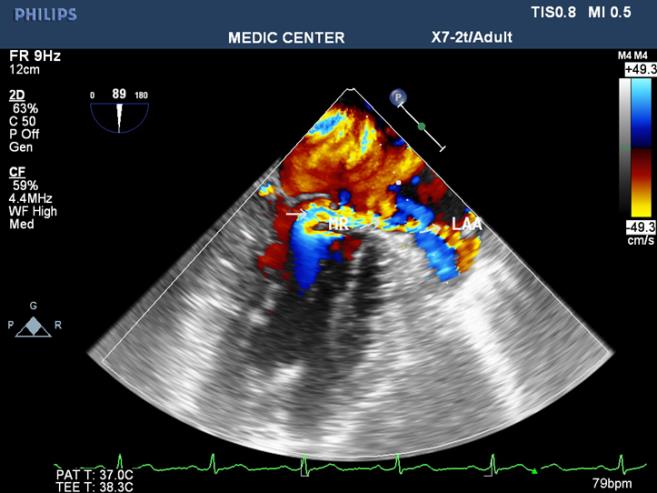
Figure 18. 2DTEE 90₀ plane visualizes a severe MR with excentric jet radiating into LAA
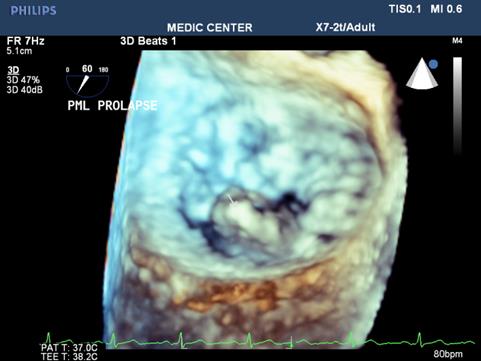
Figure 19. RT-3DTEE notes protruding PML viewed from LA side
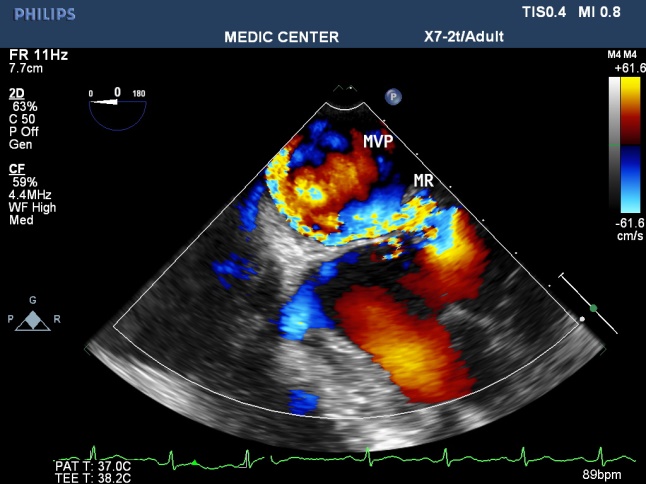
Figure 20. Excentric jet MR due to Flail MV
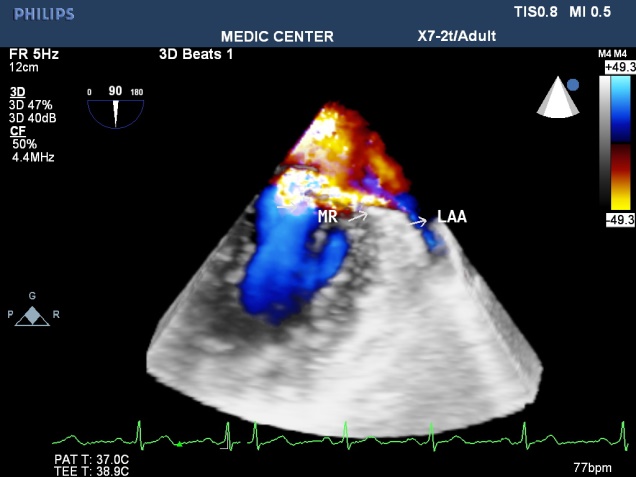
Figure 21. Live 3D shows the severe MR
Among 204 Pts with ASD, The secundum defects account for approximately 78%, then primum ASDs 6%, sinus venosus ASDs 12%, multiple shunt ASD 4%, unroofed coronary sinus not seen. 3D TEE can assess the size of ASD and the circumferential rims to select Patients for Transcatether closure. Currently we perform ASD closure limited to ASDs less than 30mm and with at least 5mm of circumferential rims (Table 1).
Table 1.
ASD
closure performed limited to ASDs less than 30mm and with at least 5mm of circumferential rims
ASD |
Ostium II |
Ostium I |
Sinus venosus |
Multiple shunt ASD |
217 |
170 |
13 |
26 |
8 |
The X-plan mode can be used to estimate the maximal diameter of defect in two orthogonal planes. Three-dimensional (3D) TEE imaging is an important adjunct to 2D imaging because multiplanar reconstruction ensures that the defect is measured accurately.
Three-dimensional (3D) TEE images can be rotated to demonstrate the defect from the RA or LA side in evaluating the secundum atrial septal defect rims. This improves understanding of their shape and relationships to surrounding intracardiac structures.
Multiple ASDs account only 4%, 3D TEE with wide sector can detect and visualize all the shunts through IAS (Figures 22-37).
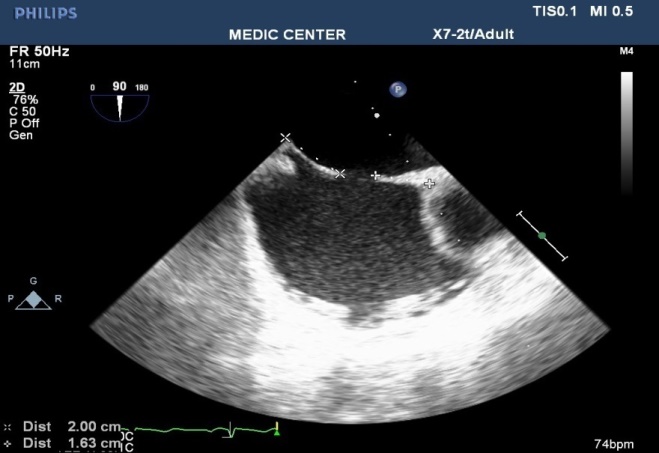
Figure 22. 2DTEE multiplane at 90⁰ ( Bicaval view ) visualizing a secundum ASD
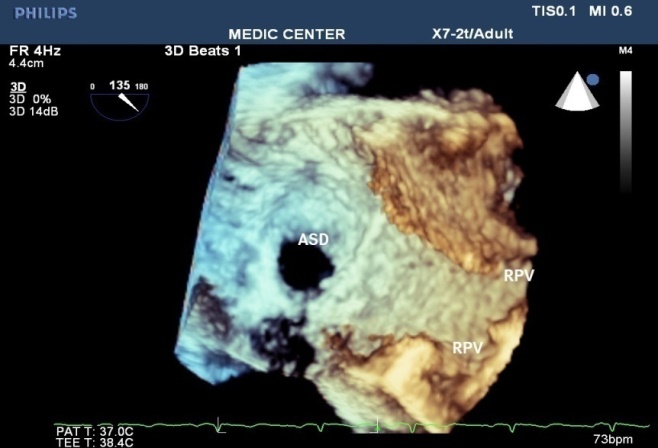
Figure 23. 3DTEE Zoom mode presenting a secundum ASD (shape, size, all rims)
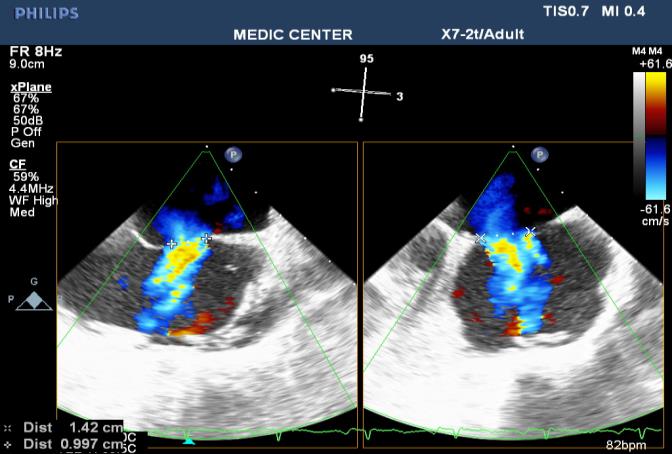
Figure 24. 2DTEE X-plane showing the L-R shunting through the secumdum ASD
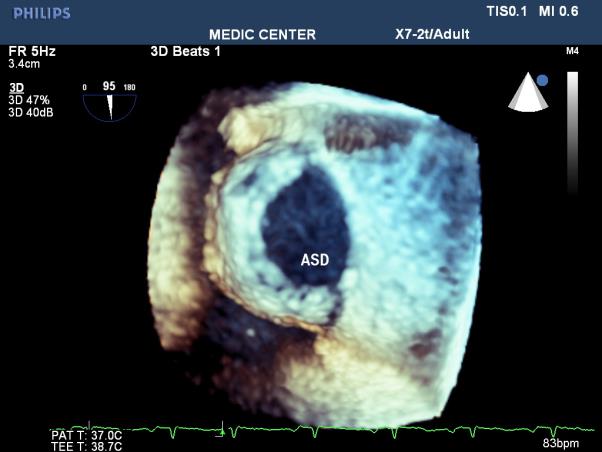
Figure 25. 3D image better demonstrates the shape and size of the secundum ASD
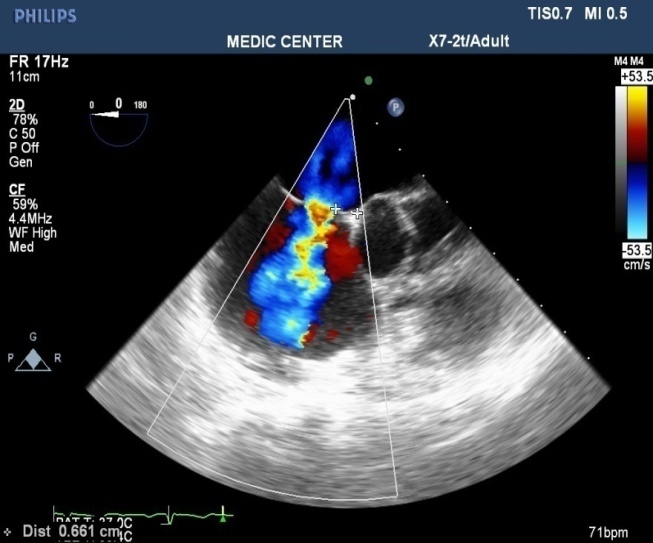
Figure 26. L-R shunting secundum ASD demonstrated with color flow imaging
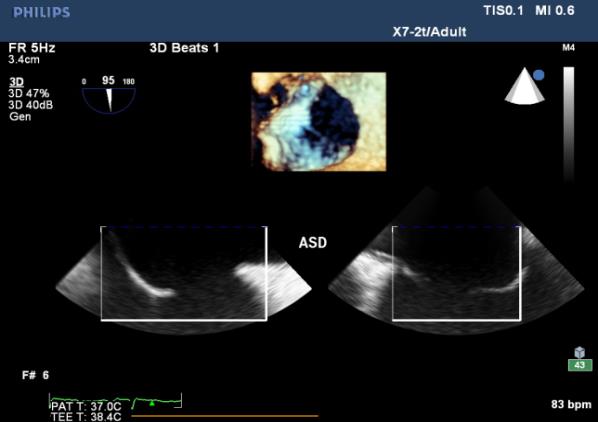
Figure 27. I crop mode showing simultaneously 3D and 2D images
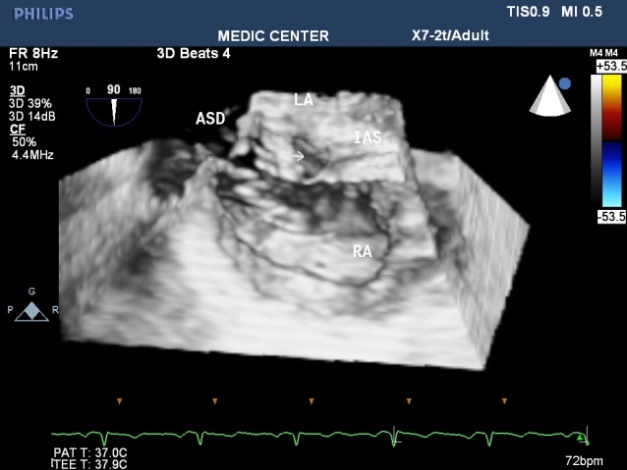
Figure 28. Multibeats live mode without color flow imaging visualizes a secundum ASD
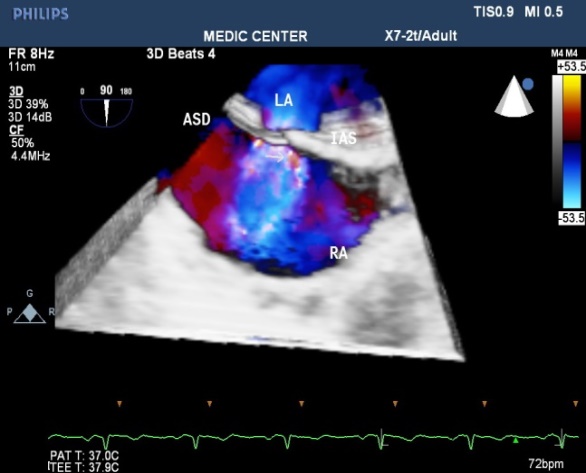
Figure 29. Multibeats live mode with color fow mapping visualizes the L-R shunt
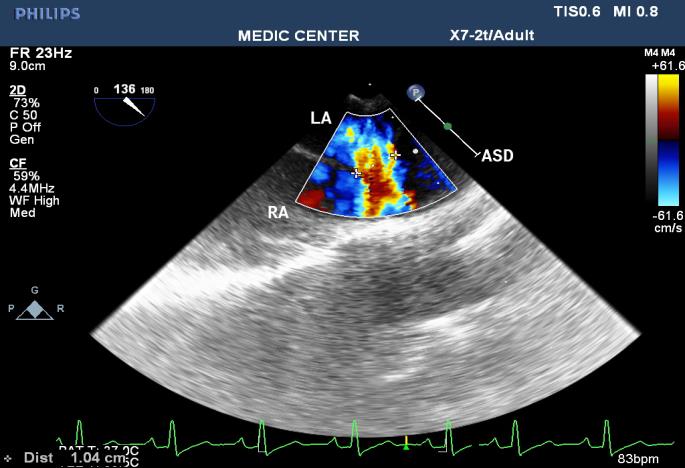
Figure 30. SVC sinus venosus ASD with L-R shunting
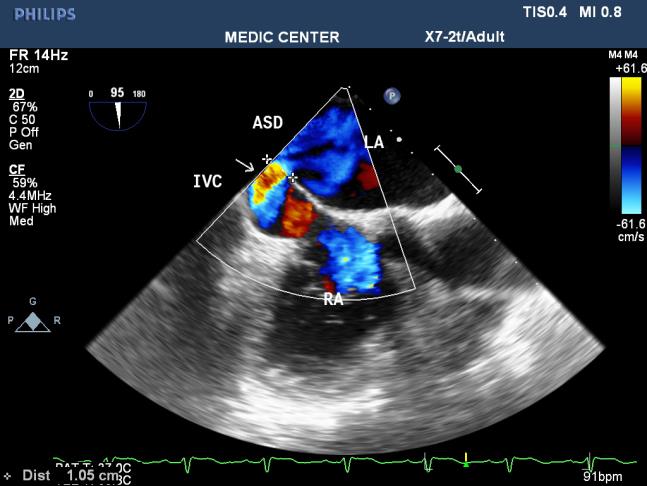
Figure 31. IVC sinus venosus ASD with L-R shunting
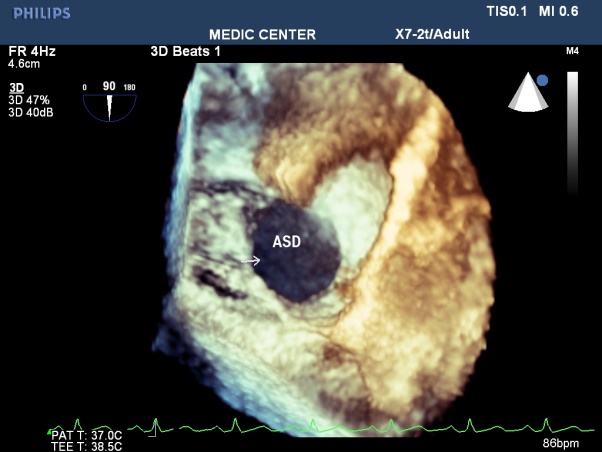
Figure 32. Secundum ASD viewed from LA
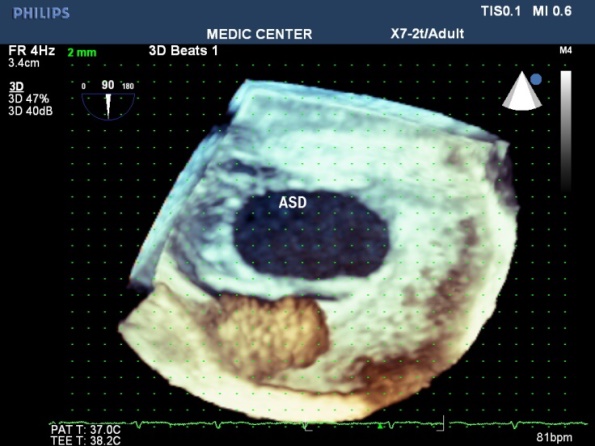
Figure 33. Secundum ASD visualized on 3DTEE Zoom mode
Figure 34. Primum ASD viewed on 2DTEE
Figure 35. Multiplane 2DTEE with color shows the papillon sign of defect
Figure 36. Primum ASD with L-R shunting seen on Live 3DTEE
Figure 37. Multiple ASD visualized from Live 3DTEE
Cardiac myxomas in our study develop in the LA, pedunculated and attached to IAS. Three-dimensional ( 3D )TEE shows the location, the size, the mobility and the stalk of myxoma on Live 3D and Full volume.
Narrowing the diagnosis down by 2DTEE and then 3DTEE should be and is the target of echocardiographic imaging.
Three dimensional 3DTEE can study the obstruction of mitral orifice caused by protruding myxoma [1-10].
Tumor of the RV and Fibroblastoma of aortic cups were noted in our study (Figures 38-43).
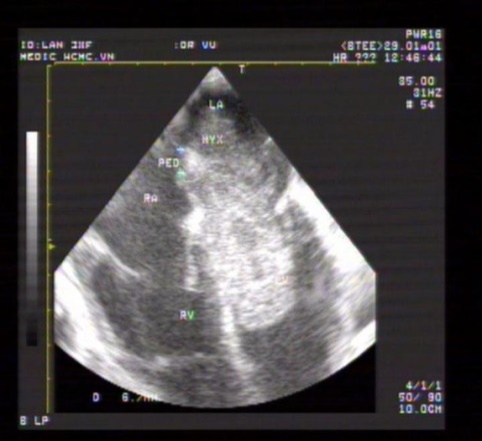
Figure 38. Giant myxoma seen on 2DTEE
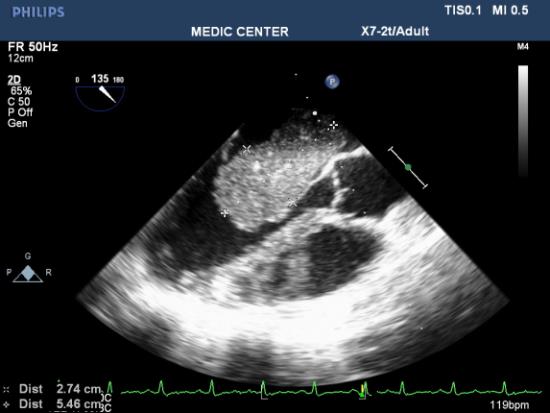
Figure 39. 2DTEE multiplane at 135⁰ shows LA myxoma

Figure 40. LA myxoma visualized on 3DTEE Live mode
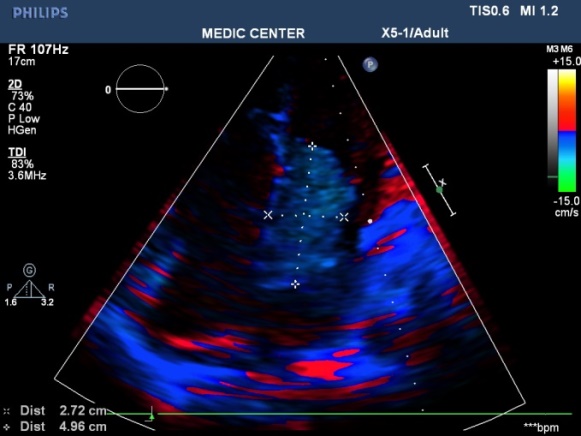
Figure 41. LA myxoma viewed on 2D TTE TDI
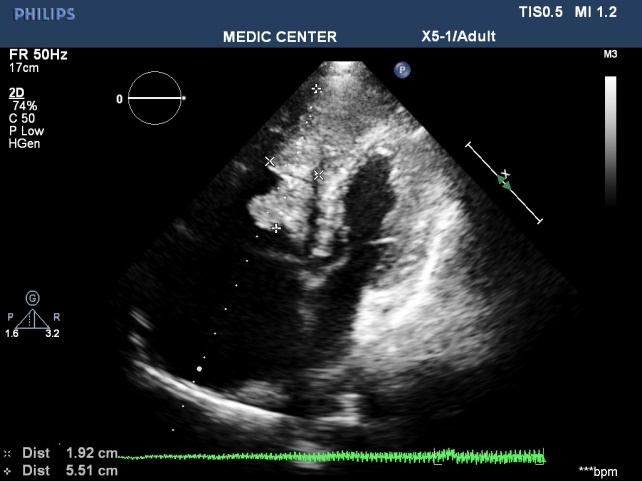
Figure 42. extensive tumor of RV detected on 2DTTE
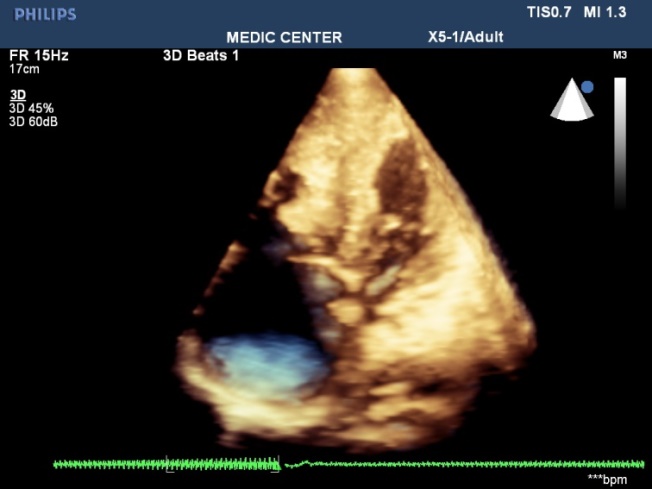
Figure 43. RV tumor viewed from 3DTTE
Endocarditis, infection of the endocardium and heart valves, the diagnosis and therapeutic of this condition has improved by echocardiography, especially TEE. Echocardiography not only provides evidence of endocardial infection as vegetation, but also offers important hemodynamic information like regurgitation severity and other structural complications.
The vegetations in our study have been found on the mitral leaflets with MVP, bicuspid aortic cusps, pulmonary valves and beside small VSD [11-17].
Among 12 cases of Infective Endocarditis, the underlying cardiac lesions includes MVP, Bicuspid Aorta, VSD and pulmonic valve stenosis (Table 2) (Figures 44-51).
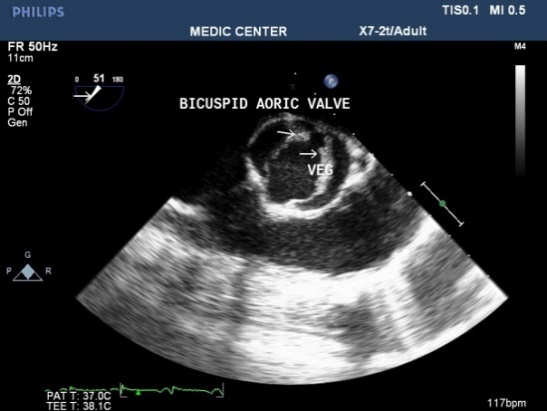
Figure 44. Bicuspid Aorta with vegetation seen on 2DTEE
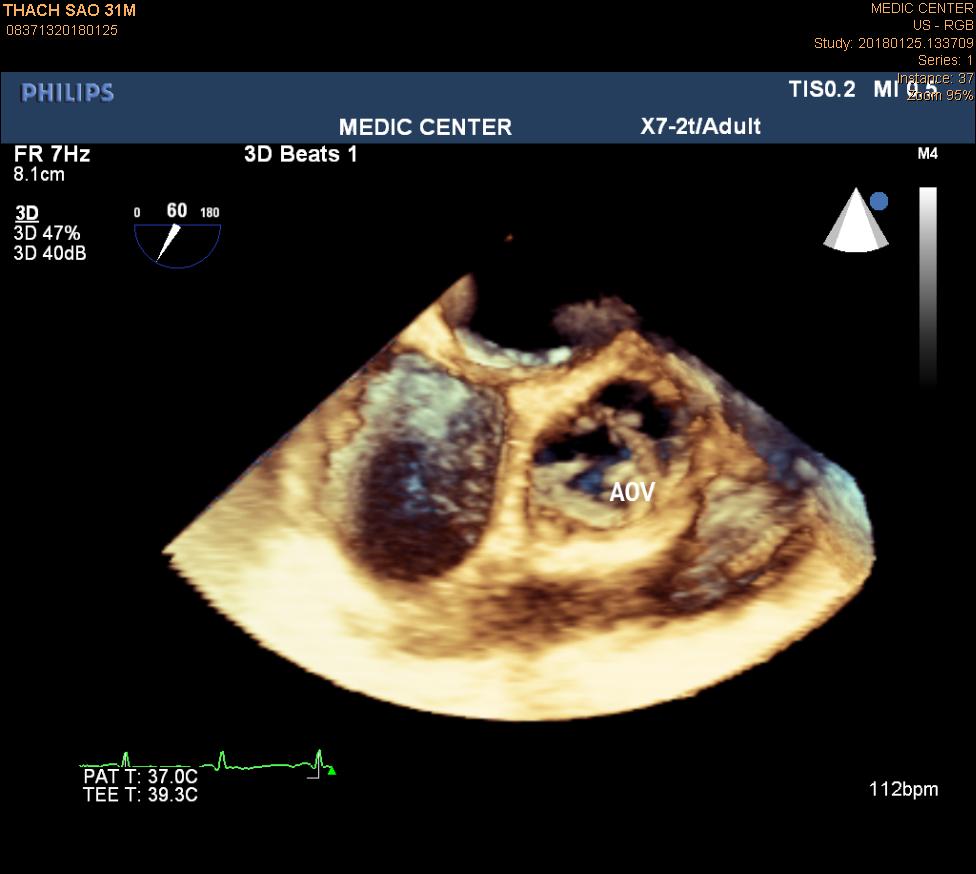
Figure 45. Bicuspid Aorta with vegetation seen on Live 3DTEE
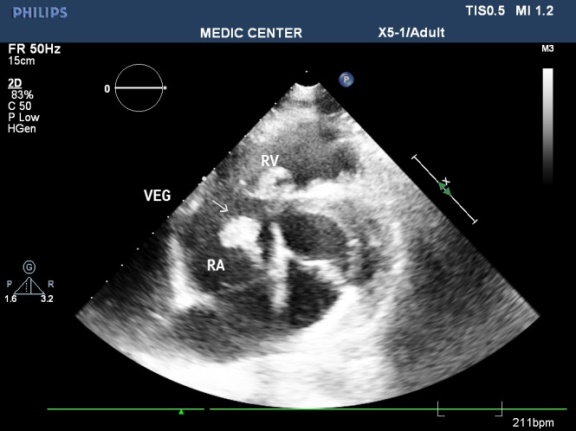
Figure 46. Vegetation seen at patient with VSD, 2DTEE imaging
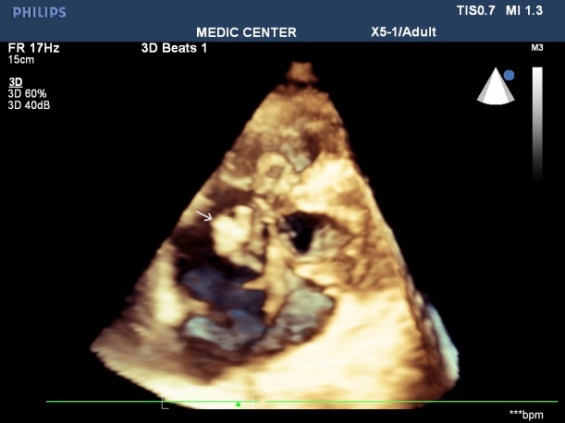
Figure 47. Vegetation seen at patient with VSD, Live 3DTEE imaging
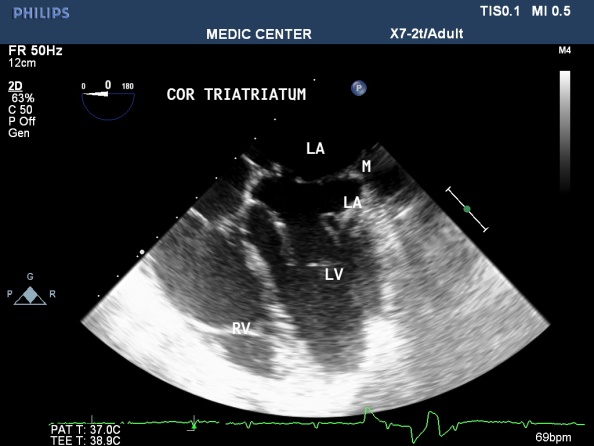
Figure 48. 2DTEE image with details of Cor Triatriatum
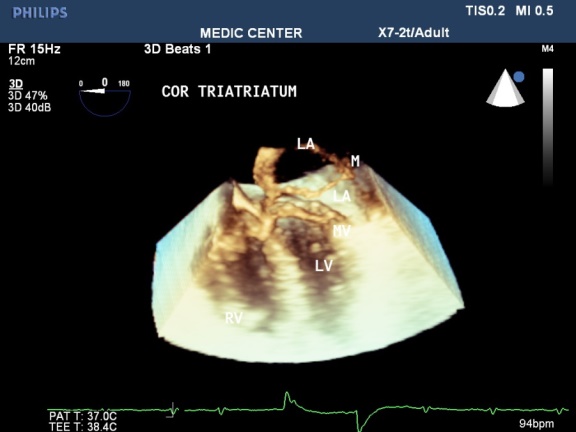
Figure 49. Live 3DTEE image showing Cor Triatriatum
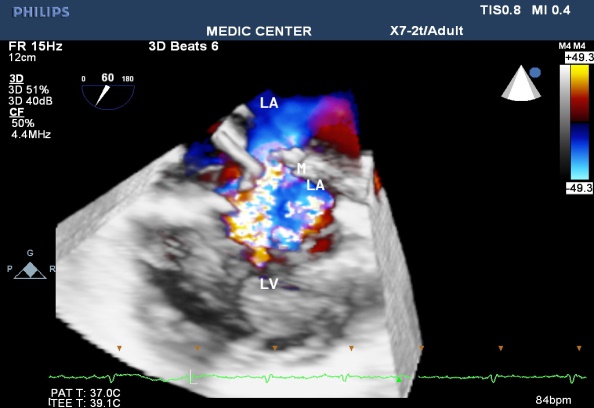
Figure 50. Cor Triatriatum with aliasing flow through the separated membrane
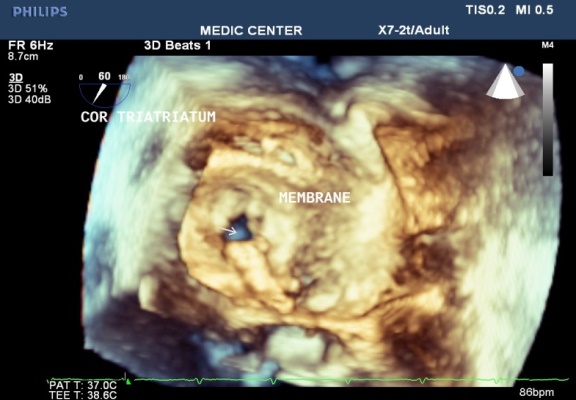
Figure 51. Cor Triatriatum viewed from LA . a small opening of membrane noted
Table 2. Among 12 cases of Infective Endocarditis, the underlying cardiac lesions includes MVP, Bicuspid Aorta, VSD and pulmonic valve stenosis
Underlying diseases |
MVP, Rheumatic MR |
Bicuspid Aorta |
VSD |
Pulmonic stenosis |
12 |
5 |
3 |
3 |
1 |
High risk of embolic events from atheromatous plaque of the Aorta: 2 cases (Figures 52 and 53).
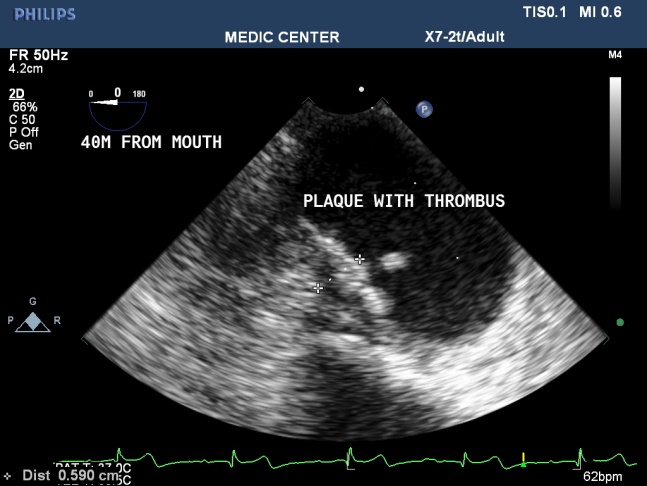
Figure 52. Atheromatous plaque of descending Aorta recorded on 2DTEE
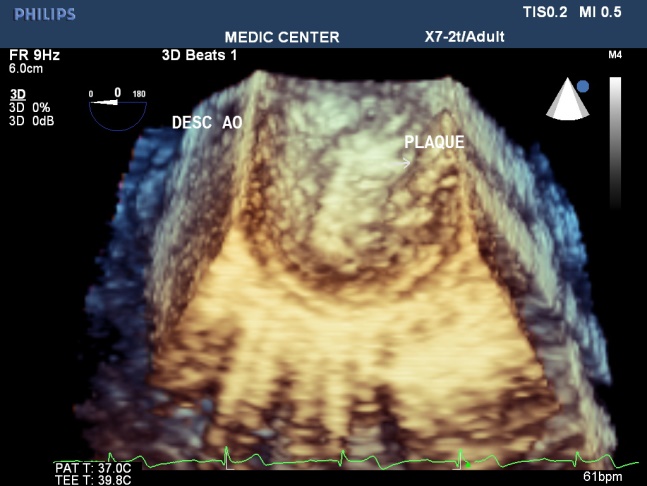
Figure 53. Atheromatous plaque of descending Aorta recorded on Live 3DTEE
Three Dimensional (3D) TEE is a novel technique that provides excellent images of the mitral valve to assess valve anatomy, evaluate the severity [15].
D. Schlosshan, et al. [6] studied 43 consecutive patients with rheumatic mitral stenosis and found that MVA3D measurements were significantly lower compare with MVA2D ( mean differnce -0.16 ± 0.22 cm2, p < 0.005 ). In our study we found MVA3D significantly smaller mean MVA2D : : mean difference= 0.21 cm2 with p<0.001.
The cropping function on 3D TEE ensures that the orifice area is measured in a plane that is at the tip of the mitral valve and perpendicular to the inflow through the valve [12].
Assessment of consequences on the LA and LAA ( study LA volume, LAA thrombi ) using X-plan function and 3D Zoom should be preferred because it is accurate and strongly related to predicting thromboembolic events and detecting thrombi [15]. Thrombi in LA and LAA were recorded on 24 patients with AF and 4 patient with sinus rhythm in our study results.
In the current area, Live 3D TEE is a usefull complementary tool in assessing the size, site, and shape of an ASD, its rims and realtions with neighboring structures. It is also helful in confirming the good positioning of a device and identifying the site of any residual shunt next to device closure [11].
We always display a true en face view of the defect from the left atrium so that its dimensions can be accurately measured [12]. Three dimensional 3D TEE visualizes clearly the shape and the rims in a view only, that previously were obtained only by many consecutive 2D views. Review of 72 suscessful cases of ASD device closure demonstrates the size of ASD and its rims were always recorded and measured on the 3D TEE view from the left atrium. Three patients with unsuscessfull ASD device closure related to short aortic rim ( from 0 to 3mm ).
Case Endocarditis of pulmonary valve is very rare one, the rough systolis murmur at left sternal border resulted in a false diagnosis of disease as small VSD. Patient then had been sent to our department one year later to pratice TTE and TEE because of fever. TTE, 2D TEE then 3D TEE consecutively was done. Vegetation of 11x5mm in size recorded from parasternal shorst axis view TTE and 2D TEE, then we found a mobile vegetation with greater size about 14x7mm associated with dilated pulmonary trunk of 35mm in diameter and a subpulmonary valve aneurys m of 25x 36mm. MDCT-640 was indicated and detected a subpulmonary valve aneurysm of 27x38mm and pulmonary trunk dilatation of 40mm in diameter. Surgical plasty of pulmonary valve and aneurysmal ressection were performed (Figures 54-57).

Figure 54. 2DTEE multiplane shows vegetation attached to pulmonary valve

Figure 55. 3DTEE better showing the shape, size and mobility of vegetation
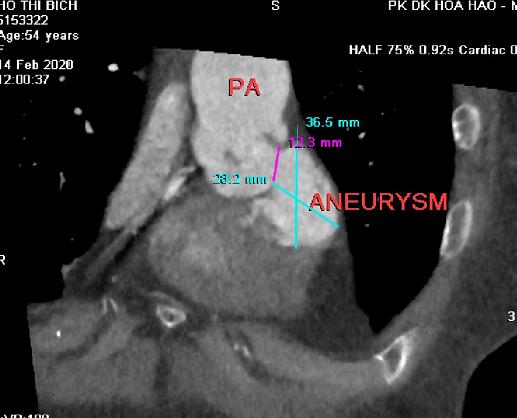
Figure 56. MDCT with MPR image visualizing a subpulmonary valve aneurysm
Figure 57. 3D Surface Display image presents an aneurysm closed to infundibulum
Melissa Lyle, et al. [4] reported a case of pulmonary valve vegetation, the patient was a old man 63 y.o, his past history included CAD status post bypass grafting with postoperative course complicated by an Enterococcus faecalis blood stream infection and aortic valve endocarditis.The Author did not explain why the vegetation attached to the pulmonary cusps from the left side as aortic valve endocarditis.
Jevon Samaroo Campbell, et al. [2] published an isolated pulmonic valve endocarditis case. The patient had no underlying valvular disease, he was later found to be bacteremic with S mitis. TEE detected a large pulmonic valve vegetation.
The majority of patients presented to be performed Three-Dimensional (3D) TEE were related to valvulopathies, especially mitral stenosis; and congenital shunts in which atrial septal defects were predominant.
Three-Dimensional (3D) TEE ensures that the orifice area is measured in a plane that is at the tip of the mitral valve. Determination of the status of commissural fusion, particularly the symmetry length of commissural fusion is valuable information to predict the success of Balloon Mitral Commissurotomy.
Three-Dimensional (3D) TEE enables improved visualization of ASDs using unique en face representation of the interatrial septum. Three-Dimensional (3D) TEE provides the valuable information including shape, size of defect, its rims prior to perform transcatether device closure.
Three-Dimensional (3D) TEE overcomes the disadvantages of other modalities like fluoroscopy, 2D TTE, 2D TEE during percutaneous interventions, for example 3D TEE is the unique modality can show the total anatomical structures in only one view.
- Blaeakley C (2018) Impact of 3D echocardiography on grading of mitral stenosis and prediction clinical events. Echoresearch and practice 5: 4105-4111.
- Campbell JS (2019) Isolated Pulmonic Valve Endocarditis. Am J Case Rep 20: 151-153.
- Izumo M (2013) Comparison of Real-Time Three-Dimensional Transesophageal Echocardiography for Quantification of Mitral Valve Prolapse in Patients with Severe Mitral Regurgitation. Am J Cardiol 111: 588-594.
- Lyle M (2018) Pulmonary Valve Endocarditis. JACC.
- http://www.jiaecho.org/article.asp?issn=25431463;year=2019;volume=3;issue=3;spage=163;epage=176;aulast=Omar
- Schlosshan D (2011) Real-Time 3D Transesophageal Echocardiography for the Evaluation of Rheumatic Mitral Stenosis. JACC Cardiovascular Imaging.
- Sharma VK (2011) Three-dimensional trans-esophageal Echocardiographic Evaluation of Atrial Septal Defects: A Pictorial Essay. Images Pediatr Cardol 13: 1-18.
- Silvestry FE (2015) Guidelines for the Echocardiographic Assessment of Atrial Septal Defect and Patent Foramen Ovale: From the American Society of Echocardiography and Society for Cardiac Angiography and Interventions. J am soc echocardiogr 28: 910-958.
- Zoghbi WA (2017) Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation. A report from the American Society of Echocardiography. Developed in Collaboration with the Society of Cardiovascular Magnetic Resonance. J Am Soc Echocardiogr.
- Armstrong WF, Ryan T (2010) Feigenbaum’s Echocardiography, 7th Edition, William &Wilkins; pp: 01-38.
- Gatzoulis MA, Webb GD, Daubenney PEF (2018) Diagnosis and Management of Adult Congenital Heart Disease, 3th Edition, Elsevier; pp: 306-315.
- Gill EA (2013) MD Atlas of 3D Echocardiography, 1st Edition, Elsevier, pp: 75-338.
- Lang RM (2012) EAE, ASE Recommendations for Image Acquisition and Display Using Three-Dimensional Echocardiography. J Am Soc Echocardiography 25: 3-46.
- Maurer G (1994) Transesophageal Echocardiography, McGraw-Hill; pp: 1-65.
- Otto C (2017) The Practice of Clinical Echocardiography, 5th Edition, Elsevier; pp 261-455.
- Roudaut R (1994) Echocardiographie Transoesophagienne, Centre Hospitalier Universitaire Bordeaux.
- Topol EJ, Paul S (2016) Teirstein.Textbook of Interventional Cardiology, 7th Edition, Elsevier, pp 727-811, 2016.