Abstract
We report a rare presentation of invasive thymoma in an otherwise well 83 year old lady. Echocardiography, cardiac MR and PET imaging revealed a right atrial mass extending to and partially obliterating superior vena cava. The differentials were cardiac lymphoma, sarcoma, metastatic tumour or thymoma. A transvenous biopsy of the right atrial mass was performed under transoesophageal echocardiography guidance. The pathology showed invasive thymoma type B3. The patient was managed with steroids, oral anticoagulation and radiotherapy.
Keywords
cardiac MRI, cardiac thymoma, right atrial mass
Introduction
Neoplastic involvement of the heart at autopsy has been reported to occur in 2% to 20% of all patients dying of malignancy [1]. Thymoma is a rare neoplasm primarily arising within anterior mediastinum. Most thymomas with cardiac involvement are limited to pericardium and very few cases of transvenous extension with intracardiac involvement have been reported [2-4]. Very few of these cases detail the use of cardiac MR, PET imaging and transoesophageal echocardiogram guided biopsy to aid in the diagnosis. This case highlights the diagnostic approach to a complex right atrial mass, the utility of multi-modality imaging and the noble finding of transvenous extension of invasive thymoma.
Case Report
An 83 year old lady who was otherwise well and independent presented to the Emergency Department with progressive dyspnoea and non-specific chest pain. There was no associated limb swelling, orthopnoea or paroxysmal nocturnal dyspnoea. On examination she was tachypnoeic but other vital signs were normal. Physical examination revealed mild facial swelling and distention of superficial veins of the anterior chest wall and external jugular veins. She had a soft systolic murmur at the left lower sternal edge. Her blood tests and ECG were unremarkable. Transthoracic and transoesophageal echocardiograms were performed which revealed a severely dilated right atrium which contained a large mobile mostly homogeneous mass attached to the right atrial free wall prolapsing through the tricuspid valve with extension into the superior vena cava.
A cardiac MR was performed to further evaluate the mass revealing a 60mm x 50mm contrast enhancing mass in the right atrium. The mass extended into the lumen of the superior vena cava all the way up to the confluence of the brachiocephalic veins. The mass was causing significant intraluminal narrowing of the superior vena cava. The intracardiac mass was associated with anterior mediastinal lymphadenopathy. The morphology, transvenous extension and signal characteristics most favoured of a diagnosis of lymphoma. However, a PET scan showed intense FDG-activity of the mediastinal and right atrial masses suggestive of malignant thymoma[Figure 1,2 and 3]. Since histologic examination was unavailable to guide the treatment we decided to perform a biopsy of right atrial mass. A transoesophageal echocardiogram guided transvenous biopsy of right atrial mass revealed B3 thymoma.

Figure 1. Contrast enhanced CT scan coronal reformat image showing extension of mass from the right atrium to the superior vena cava.
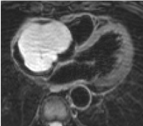
Figure 2.Axial T2 dark blood image showing the mass expanding the right atrium and abutting the tricuspid valve leaflets.
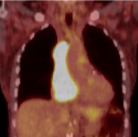
Figure 3.FDG-PET CT scan fused coronal image shows that the mass has intense FDG uptake.
Following multidisciplinary discussion it was decided that the patient would not be suitable for surgery and the optimal management option was for a short course of steroids and radiotherapy with prophylactic anticoagulation. Following radiotherapy her symptoms were markedly improved with associated reduction in thymoma size on CT scan. The patient is currently being observed with repeat CT scanning.
Discussion
Invasive thymoma with cardiac involvement is a rare and poorly described entity with a wide range of possible initial presentations. The presentations may involve symptoms of superior vena cava obstruction or cardiac tamponade or myocarditis [5]. It is evident from this case that investigation of cardiac masses is required with imaging studies such as cardiac MR and biopsy to determine the origin and aetiology to guide multidisciplinary management.
Conclusions
This case describes a case of a rare invasive thymoma with cardiac involvement that was not suitable for surgical management and required radiotherapy with some response.
Funding
No funding was required for this case report
Competing Interest
The authors declare that they have no competing interests
References
2021 Copyright OAT. All rights reserv
- Weinberg BA, Conces DJ, Waller BF (1989) Cardiac manifestations of noncardiac tumors. Part I: Direct effects. ClinCardiol12:289-296.
- Kurata A, Saji H, Ikeda N, Kuroda M (2013) Intracaval and intracardiac extension of invasive thymoma complicated by superior and inferior vena cava syndrome. PatholInt63:56-62.
- Dib HR, Friedman B, Khouli HI, Gerber DR, Weiss RL (1994) Malignant thymoma. A complicated triad of SVC syndrome, cardiac tamponade, and DIC. Chest105: 941-942.[Crossref]
- Odim J, Reehal V, Laks H, Mehta U, Fishbein MC (2003) Surgical pathology of cardiac tumors: two decades at an urban institution. Cardiovascular Pathology12:267-270.
- Kamiya H, Yasuda T, Nagamine H, Sakakibara N, Nishida S, et al. (2001) Surgical treatment of primary cardiac tumors. Japanese circulation journal65:315-319.