ergotamine, temporal arteritis, tongue necrosis
Unexpected sudden onset of tongue necrosis is an alarming rare complication of giant cell arteritis which encompasses both temporal arteritis and rheumatic polymyalgia [1,2]. Historically, the majority of patients with temporal arteritis who develop tongue necrosis had exposure (ingestion) to ergotamine tartarte for severe migraine-like headaches [1,3-7]. Diagnosis of temporal arteritis can be challenging at times as the diagnosis of temporal arteritis has been made in some cases after tongue necrosis manifested itself as the initial presentation following ergotamine ingestion.
Ergotamine tartrate is a serotonin 1A and 2A receptor agonist medication belonging to a group of drugs known as ergot alkaloids [8-12]. This medication is used as an oxytocic agent for acute management of migraine headaches that has already begun. Ergotamine tartrate with its serotonin 2A and alpha-adrenergic activity causes coronary and peripheral arterial constriction. For acute migraine treatment its vasoconstrictor properties, reverses vasodilation that occurs over the dura and meninges in the acute migraine headache. It is not prescribed for prevention of migraine headaches. Ergotamine tartrate without or without caffeine is still prescribed and available in oral (sublingual) and suppository, and while there are many side effects associated with this medication necrosis of the tongue is not listed because of its rarity and its strong association with simultaneous presence of temporal arteritis [13-15]. It is proposed the pharmacologic vasoconstriction effect on an inflamed artery causes severe vascular compromise with subsequent soft tissue avascular necrosis. This case report discusses this rare complication in a patient who initially presented with tongue paralysis which progressed to tongue necrosis. The diagnostic workup lead to the discovery of temporal arteritis. No identifiable exposure to ergotamine tartrate was found to serve as a diagnostic clue.
A 73-year old Caucasian female with a two-week history of oral dysphasia secondary to paresthesia and paralysis of the tongue bilaterally was admitted for IV fluid hydration and evaluation. This patient nine years earlier was diagnosed with a large cell carcinoma of the right lung and underwent a right lobectomy with postoperative radiation and chemotherapy therapy. On admission (hospital day 1) the patient underwent an MRI of the head which was normal showing only small vessel changes consistent with aging. The brainstem was normal with no abnormality that could adversely impact cranial nerve 12 (hypoglossal nerve) bilaterally.
On hospital day 2 the patient underwent a CT scan with contrast of the maxillofacial region and neck given her history of malignant disease in the distant past. A nonspecific decreased attenuation of the midportion of the tongue superiorly was seen supportive of edema and/or glossitis. No other abnormal findings were found. A carotid Doppler was performed and was normal. Fluoroscopy guided lumbar puncture was also performed which showed normal cerebral spinal fluid and cultures were eventually found to be negative for bacteria or other pathogens. (Figures 1 and 2).
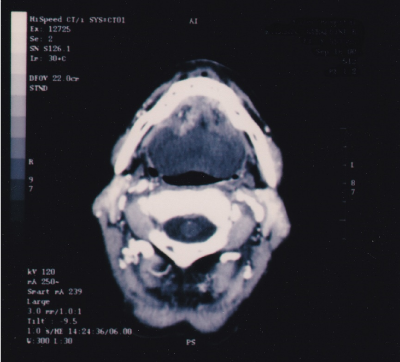
Figure 1. Maxillofacial computed tomography scan, axial view frame, showing decreased attenuation of the tongue which correlated eventually to the clinical appearance of tongue necrosis. No findings suggestive of abscess formation, cellulitis, or malignant neoplasia is demonstrated.
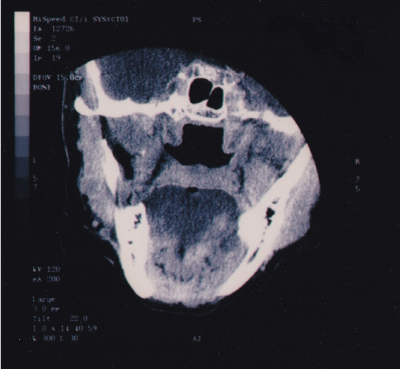
Figure 2. Maxillofacial computed tomography scan, coronal view frame, showing decreased attenuation of the tongue which correlated eventually to the clinical appearance of tongue necrosis.
On hospital day 3 the patient developed sudden loss of vision involving the right eye with no light perception. The left eye visual acuity was 20/20 with near card. Laboratory blood testing results showed SMAC, CBC, C-3 and C-4 complement, P- and C – ANCA, and ANA having normal values. Rheumatoid factor was positive with a normal level, less than 1:2. ESR was 50 mm/hr. and C-reactive protein was 15.3 (normal less than 0.5mg/dl). Repeat ESR was 54mm/hr.
High-dose parenteral corticosteroid therapy was started with methylprednisolone. The patient subsequently developed necrosis of the superficial surface of the middle to anterior dorsum of the tongue. No intervention was required with healing occurring by secondary intention. Tongue necrosis was presumedly due to avascular necrosis of the tongue soft tissues compromised by arterial blood vessel inflammation associated with giant cell arteritis affecting the head and neck region. A temporal artery biopsy was performed which was positive for the typical findings associated with temporal arteritis.
While rare elderly patients who develop acute tongue necrosis without a history of malignant neoplasia, suspicion for temporal arteritis should be included in the differential diagnosis, especially if there is exposure to ergotamine tartrate medication. This patient initially presented with bilateral tongue paresthesia and paralysis without tongue necrosis and had a distant history of malignant disease. The patient subsequently developed the feared complication associated with temporal arteritis with complete blindness of the right eye leading to endeavors to the diagnosis of temporal arteritis. Tongue necrosis manifested itself temporally just after development of complete loss of vision in the right. Because of the rarity of this complication and the wide variation in presentation in patients with giant cell arteritis/temporal arteritis diagnosis can be challenging initially. Implementing high-dose corticosteroid therapy even when there is not a definitive diagnosis and suspicion may be low appears to be a prudent course of action given its low morbidity and potential benefit.
- Llorente Pendas S, DeVicente Rodriguez JC, Gonzalez-Garcia M (1994) Tongue necrosis as a complication of temporal arteritis. Oral Surg Oral Med Oral Path 78: 448-451.
- Marcos O, Cebrecos AI, Prieto A, Sancho de Salas M (1998) Tongue necrosis in a patient with temporal arteritis. J Oral Maxillofac Surg 56: 1203-1206. [Crossref]
- Stoebner PE, Gaspard C, Meynadier J, Meunier L (1999) Tongue necrosis provoked by ergotamine tartrate and disclosing a giant cell arteritis. Eur J Dermatol 9: 652-653. [Crossref]
- Vazquez-Doval J, Martinez-vila E, Legarda I (1994) Tongue necrosis secondary to ergotamine tartrate in a patient with temporal arteritis. Arch Dermatol 130: 261-262.
- Constant E, Wolpaw JR, Brotten JL, Martin HL (1974) Tongue necrosis attributed to ergotamine in temporal arteritis. Plast Reconstr Surg 53: 241
- Bondeson J, Ericsson UB, Falke P, Mattiasson I, Nyman U, et al. (1992) Tongue necrosis in temporal arteritis provoked by ergotamine. J Intern Med 232: 541-544. [Crossref]
- Wolpaw JR, Brottem JL, Martin HL (1973) Tongue necrosis attributed to ergotamine in temporal arteritis. JAMA 225: 514-515. [Crossref]
- Graham JR, Wolff HG (1938) Mechanism of migraine headache and action of ergotamine tartrate. Arch NeuroPsych 39: 737-763.
- Young WB (1997) Appropriate use of ergotamine tartrate and dihydroergotamine in the treatment of migraine: current perspectives. Headache 37 Suppl 1: S42-45. [Crossref]
- Spierings EL (2001) Mechanism of migraine and action of antimigraine medications. Med Clin North Am 85: 943-958. [Crossref]
- Silberstein SD, Young WB (1995) Safety and efficacy of ergotamine tartrate and dihydroergotamine in the treatment of migraine and status migrainosus. Working Panel of the Headache and Facial Pain Section of the American Academy of Neurology. Neurology 45: 577-584. [Crossref]
- Baron EP, Tepper SJ (2010) Revisiting the role of ergots in the treatment of migraine and headache. Headache 50: 1353-1361. [Crossref]
- https://www.webmd.com/drugs/2/drug-6780/ergotamine-tartrate-sublingual/details
- http://www.migergot.com/
- Meyler WJ (1996) Side effects of ergotamine. Cephalalgia 16: 5-10. [Crossref]